
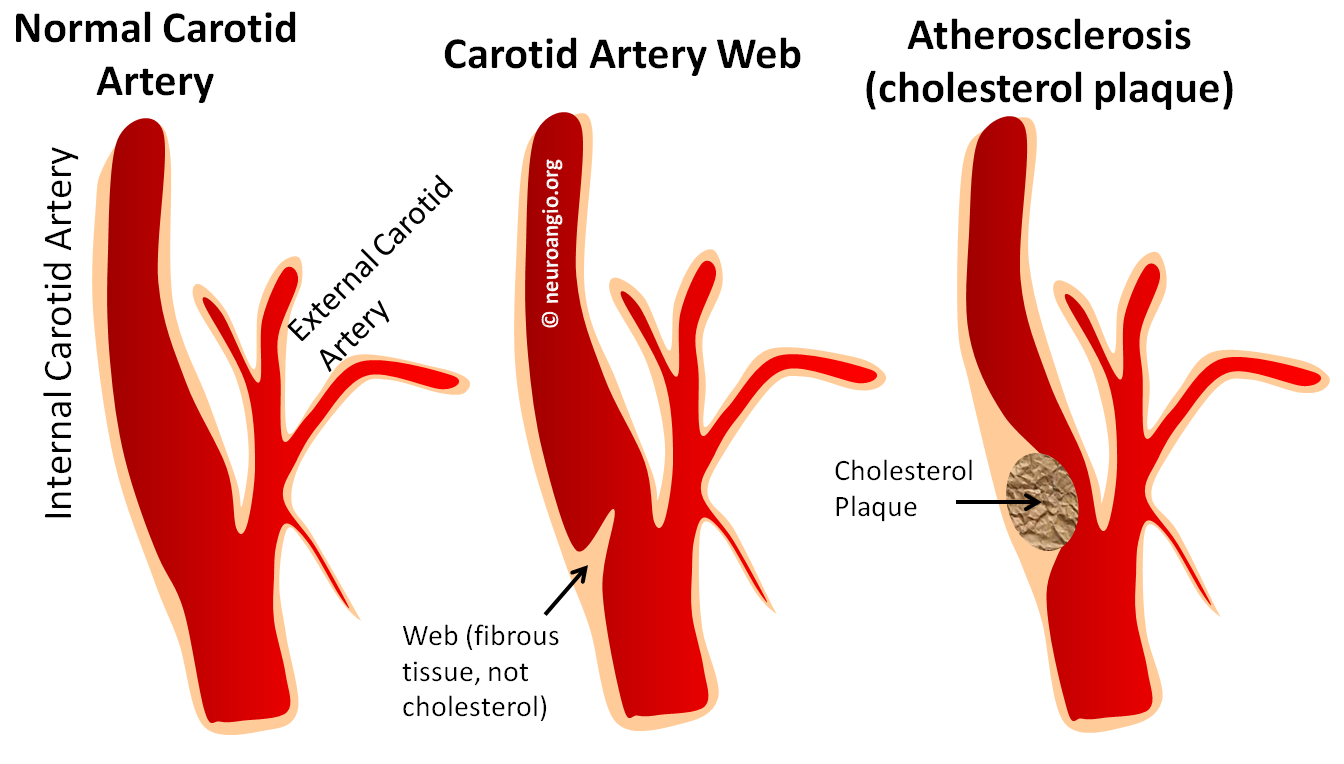
The Carotid Artery Web, or Carotid Web, is a rare and, therefore, frequently misdiagnosed condition. It is a narrowing of the carotid artery in the neck, where the common carotid artery splits (bifurcates) into the internal carotid artery which supplies the brain, and external carotid artery which supplies everything else in the head (face, throat, skin, skull, etc). Most people are familiar with the very common condition of carotid artery narrowing (stenosis). In the vast majority of people, it is caused by buildup of cholesterol in the wall of the carotid artery, usually the internal carotid artery. The usual risk factors (high blood pressure, high cholesterol, diabetes, smoking) are responsible for this kind of cholesterol plaque buildup. The plaque is a potential cause of stroke, which can happen either because the plaque gets so big that the carotid artery becomes too narrow or closes completely or, more commonly, because the plaque ruptures and pieces of it float upstream into the arteries of the brain. These pieces, or “emboli” lodge in brain arteries and block blood flow. Recent advances in stroke care make it possible to remove these emboli and restore blood flow to the brain. However, this typically has to be done extremely quickly after onset of stroke symptoms, because the brain usually cannot survive for more than a few hours with a blocked artery. That’s why it is essential to call 911 or get to the hospital as soon as possible after a suspected stroke. Many people do not know that they are having a stroke; instead, someone who is with them has to recognize the symptoms and get help.
The carotid web can also cause a stroke. However, it is different from cholesterol plaque. There is no cholesterol in the web. It is a shelf-like protrusion into the carotid artery caused by having too much “connective tissue” sticking out into the carotid artery lumen. It is not a cancer and it does not keep growing. Its as though the body decided to build a shelf or a web to partially block the lumen of the carotid artery (middle picture). Many people believe, as we do, that the web is a variant of condition called “Fibromuscular Dysplasia” As you can see, it looks different from the usual cholesterol plaque. Usually, the artery is not narrowed enough to cause a problem like a stroke. However, it does affect blood flow in the carotid artery. Sometimes, the blood flow behind the web is too slow and clots form there. These clots can then float into the brain, just like for people with cholesterol plaques in their arteries, and cause a stroke. How often this happens is not really known because the web is a much less common thing than cholesterol plaque. Nevertheless, we see these kinds of strokes a few times a year. Another page on the Carotid Web, more geared towards professionals, is here
The things to remember about the Web are:
- It is not a cholesterol plaque. People are born with the web. It is also not a dissection. Dissections usually happen in a different part of the carotid artery. See Dissection page for more information
- The web can be seen in young people who do not have the usual risk factors for vascular disease (hypertension, high cholesterol, smoking, diabetes). While it is critical to treat these factors when they exist, if a lesion such as the web is found and there are no other risk factors, then there is no reason to chase the idea of high cholesterol and concentrate on management of the web
- Most webs seem to be asymptomatic and do not cause strokes. We usually recommend that patients with a web take a baby aspirin (81 mg in the USA, 50 mg in many other countries) to lower the risk of clots forming near the web
- If a web is found to have caused a stroke, what to do is not well agreed upon because the web is not very common. Some suggest to take aspirin (if the person was not taking aspirin before the stroke). Others feel that it is not enough and that the mechanism for stroke (slow flow of blood behind the web) is not well managed by aspirin. They suggest a blood thinner like Coumadin or other, newer agents. Yet others believe that webs which cause strokes should be treated by either Carotid Artery Endarterectomy (CEA, a surgery to remove the web) or Carotid Artery Stenting (CAS). There is no trial to tell us what is the right approach because the web is rare, so we rely on experience and intuition. Our approach is to treat webs that have not caused a stroke with a baby aspirin and either do Carotid Artery Stenting or Carotid Endarterectomy for those who have had a stroke. We believe that aspirin is not strong enough for those who have had a stroke and long term anticoagulation such as Coumadin is, over years, more risky than either CEA or CAS.
- The important thing to remember is that most carotid disease is caused by a cholesterol plaque. However, webs do exist and are under-recognized and often mis-diagnosed for plaques or dissections. They look different from carotid plaques or dissections however, and are not caused by cholesterol buildup. They do not require, in our opinion, as close monitoring as cholesterol plaques do, because they are static and not progressive.
So, if you have high cholesterol, high blood pressure, smoke, etc and have carotid artery stenosis, chances are its cholesterol, and you better be good and take your medicine. However, if you do not have cholesterol, pressure, etc. issues and have a carotid stenosis that looks like the web picture above, perhaps it is a web. Many doctors or medical professionals have not heard of the web and you may need to educate them.
Illustrations
Case 1: This person had the web, initially misdiagnosed as a disssection, followed by every imaging modality available. It is a nice illustration of what a web looks like on Ultrasound, CTA, MRA (contrast and noncontrast) and finally catheter angiography.
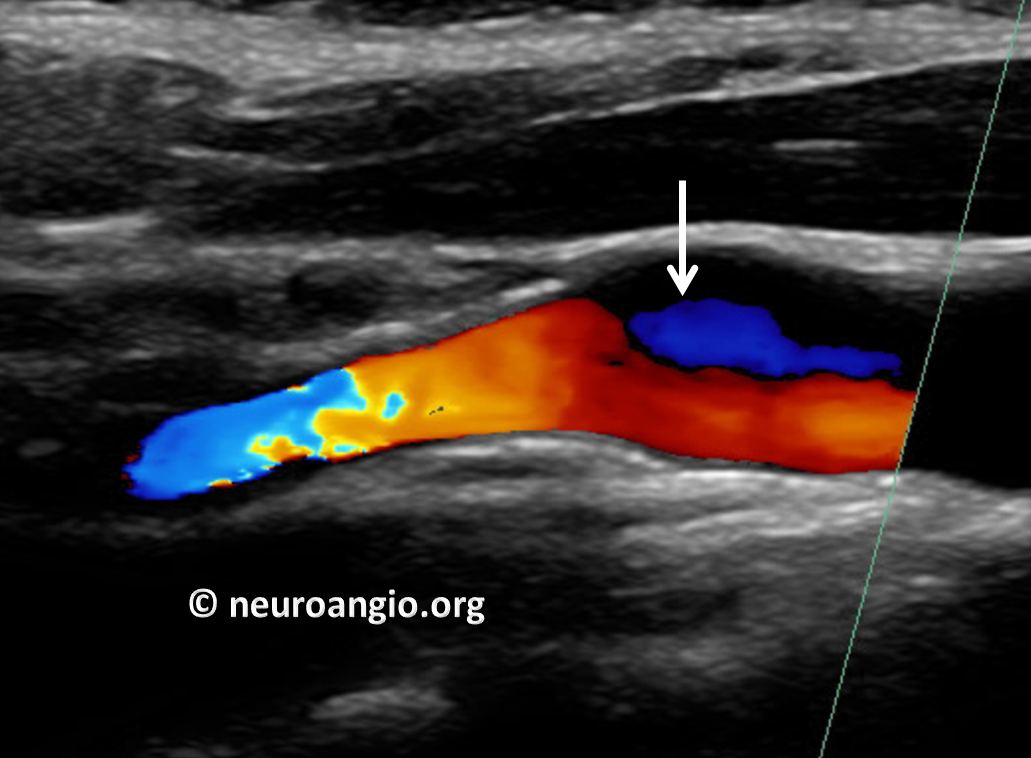
First came the Carotid Duplex. Because it relies heavily on flow, the web can be difficult to differentiate from cholesterol plaque on duplex. A flow change is seen (white arrow)
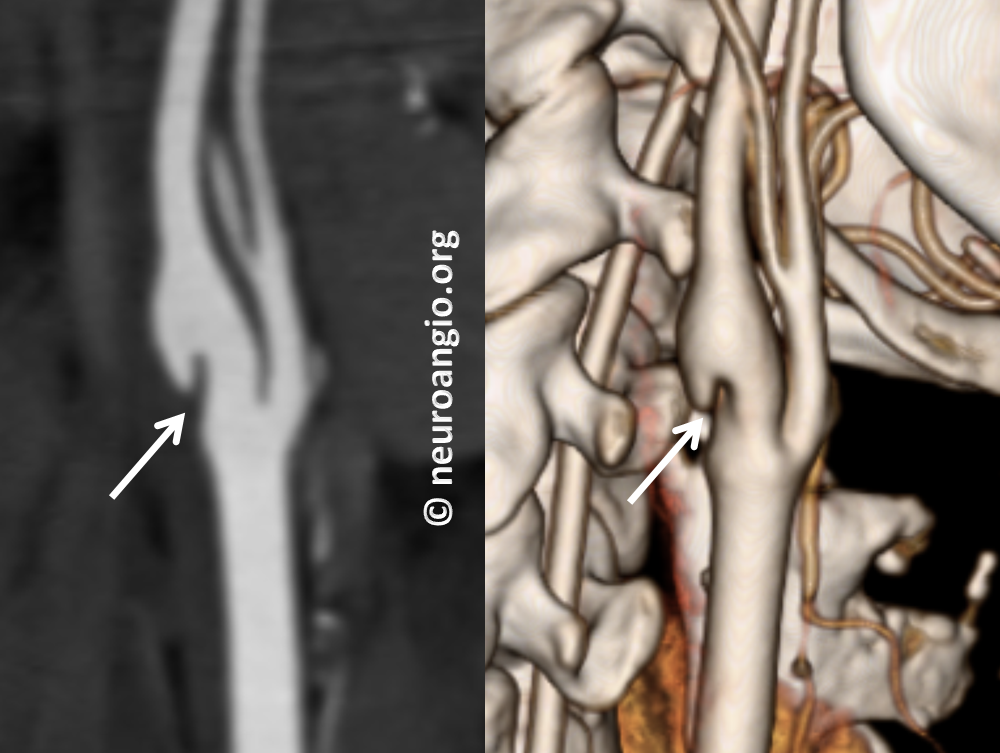
Then came CT Angiography (CTA), where the web is beautifully seen. It is an excellent way to look at the Web, but requires administration of nonionic iodine-based contrast and radiation
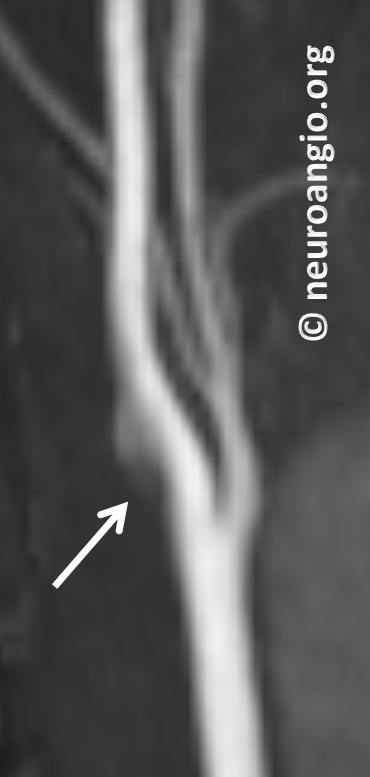
Then came noncontrast MRA. Again, this is TOF (Time of Flight) technique which relies on flow-related enhancement. Because flow in the back of the web is slow, it is not well seen on MRA. So, it is not very helpful differentiating web from atheromatous disease here
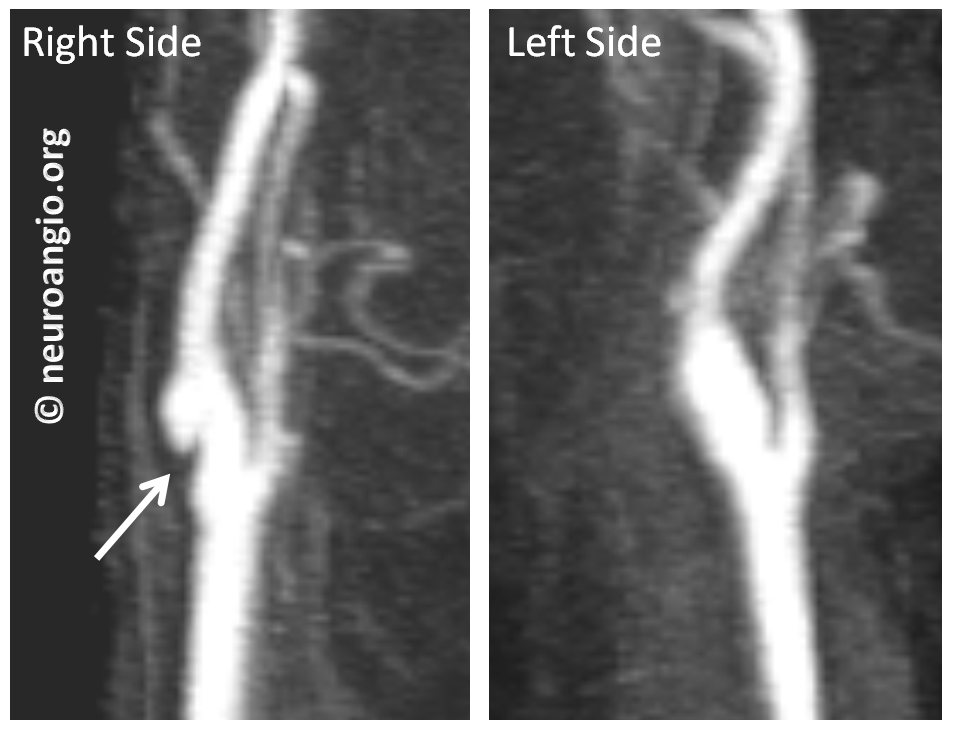
Next came contrast-enhanced MRA. Not as good as CTA here, but definitely good enough. It is our preferred method for following webs, as no radiation is involved. The left side is normal
Finally, because of another question (possible aneurysm) the patient underwent a catheter angiogram. It shows the web best, of course. However, it is minimally invasive and we do not do angiograms for webs — a CTA or contrast MRA is sufficient. This angiogram was done for another reason
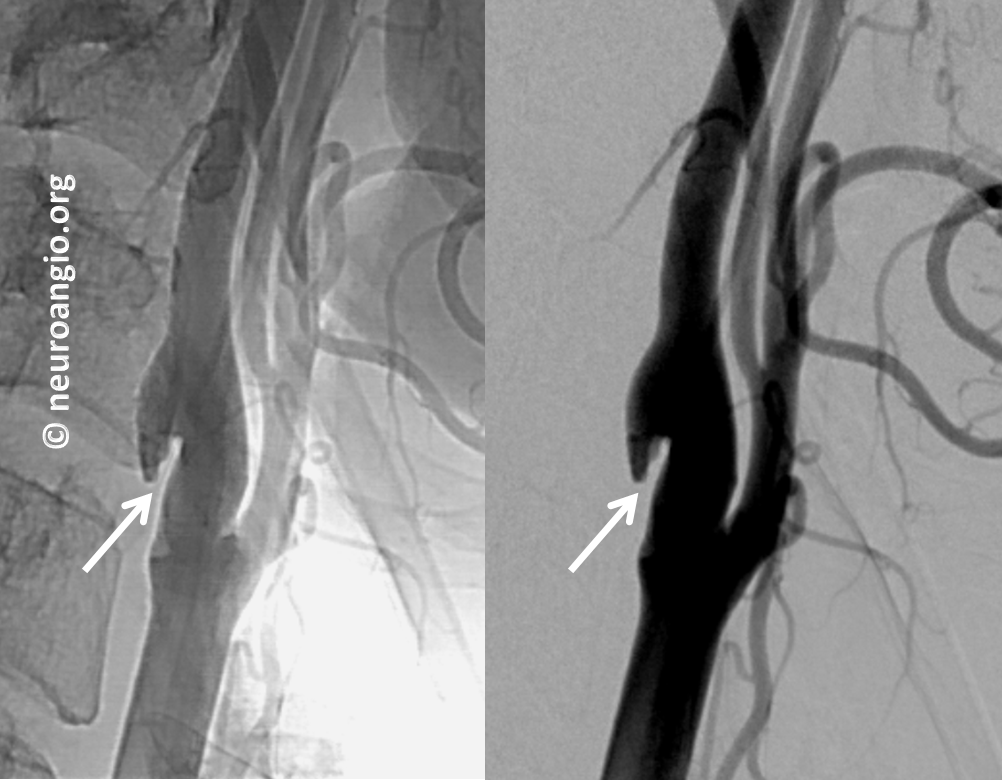
Late phase image (right) shows marked stagnation behind the web (black arrow)

This is not a dissection and not a plaque. Management is with a baby aspirin since there is no history of stroke.
Case 2 – another person. Typical images of a carotid web on an MR angiogram

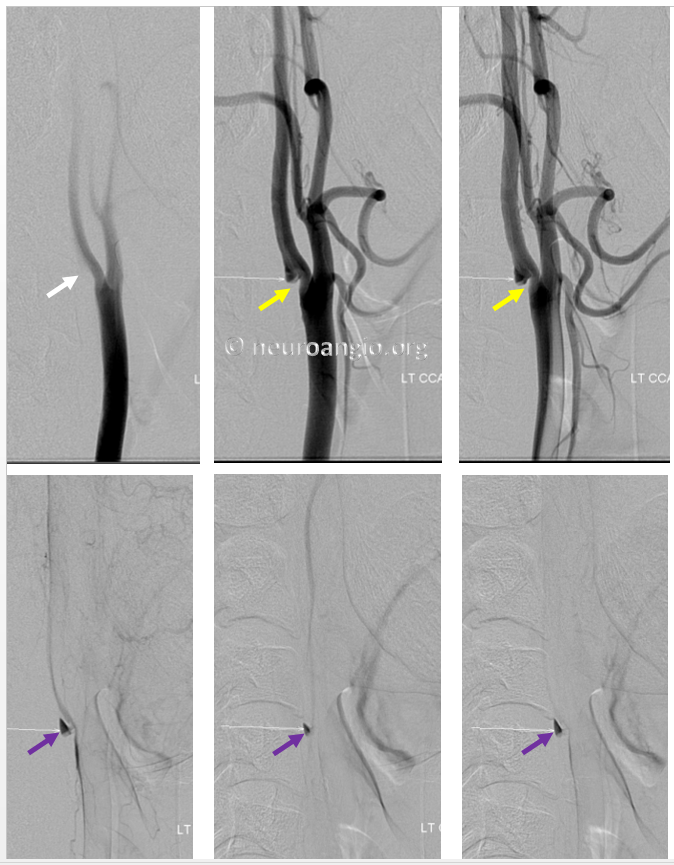
Here is a web on a catheter angiogram. The yellow arrow points to the web. The purple arrow points to slow blood flow behind the web. Clots can form in the area of slow flow (purple arrows)
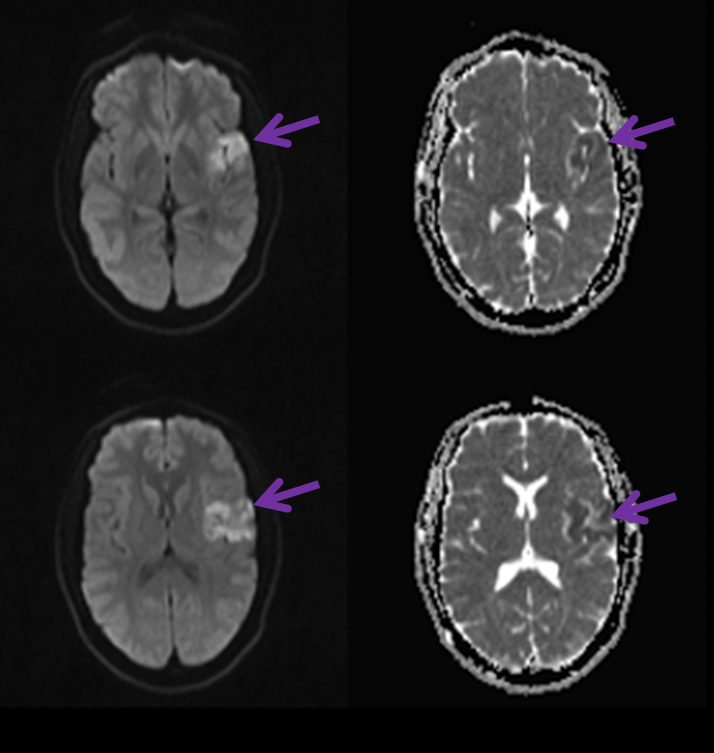
Below is an MRI of this patient how suffered a small stroke (purple arrows) because of a web.
Here is another picture of the web on an angiogram

As you can see, the webs look pretty much alike in most cases.
Atherosclerosis (Cholesterol Plaque)
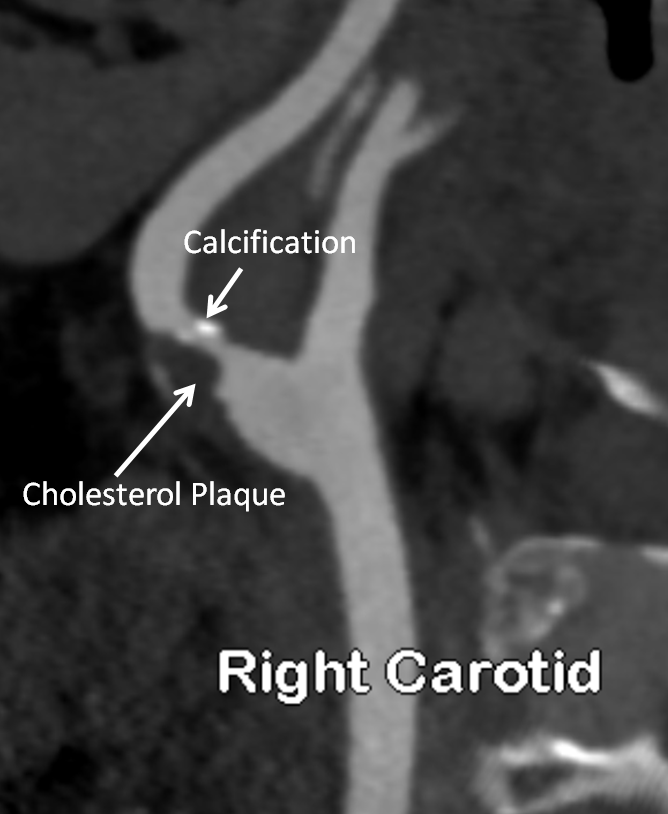
Below, on the other hand, are typical images of a patient with carotid stenosis due to a cholesterol plaque. It looks very different. The narrowing is not shelf-like, and there are areas of calcification which are usually seen in cholesterol lesions but not with the web
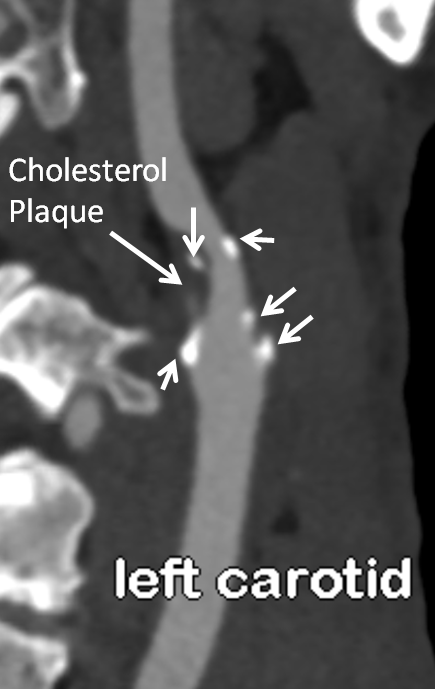
The left side of the same person shows a similar kind of situation, with a bit more calcium
Did we make all of this up? No, not really. But you decide. Here is some very legitimate literature from reputable journals about his web business. You can feel free to share them with medical professionals. You can google “Carotid Artery Web” to find these and other generally reputable sources
https://www.ncbi.nlm.nih.gov/pubmed/1987677
http://www.ajnr.org/content/early/2015/07/30/ajnr.A4431
http://pubs.rsna.org/doi/abs/10.1148/radiographics.11.3.1852941
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4638369/
http://journals.sagepub.com/doi/abs/10.1177/1591019916633245