Very commonly in our practice, intracranial stenting is done in hyperacute phase, during acute ischemic stroke, when the vessel is closed and should be opened. SAMMPRIS does not apply in this setting and it is now abundantly clear that during acute occlusion stenting is clearly beneficial.
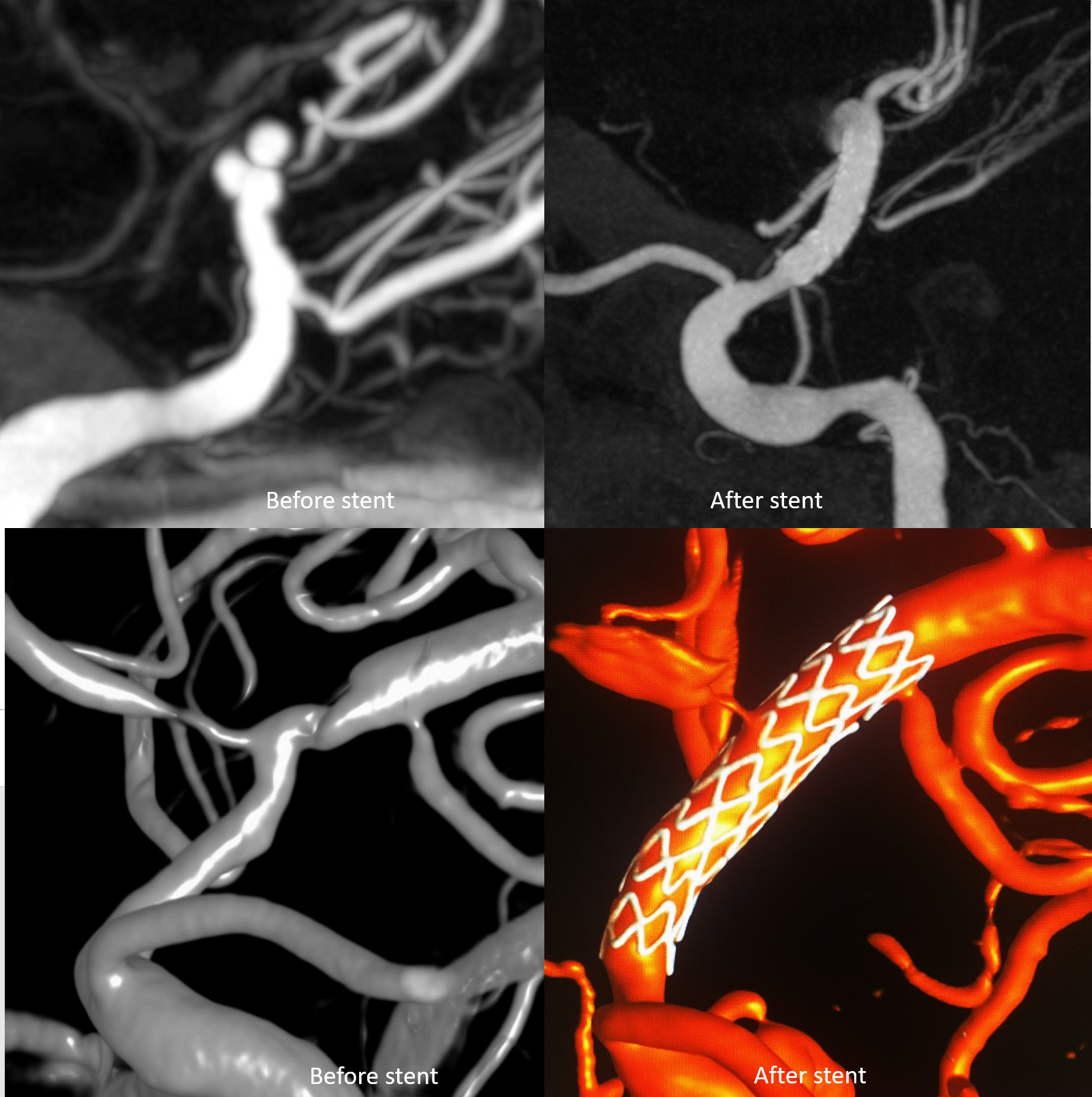
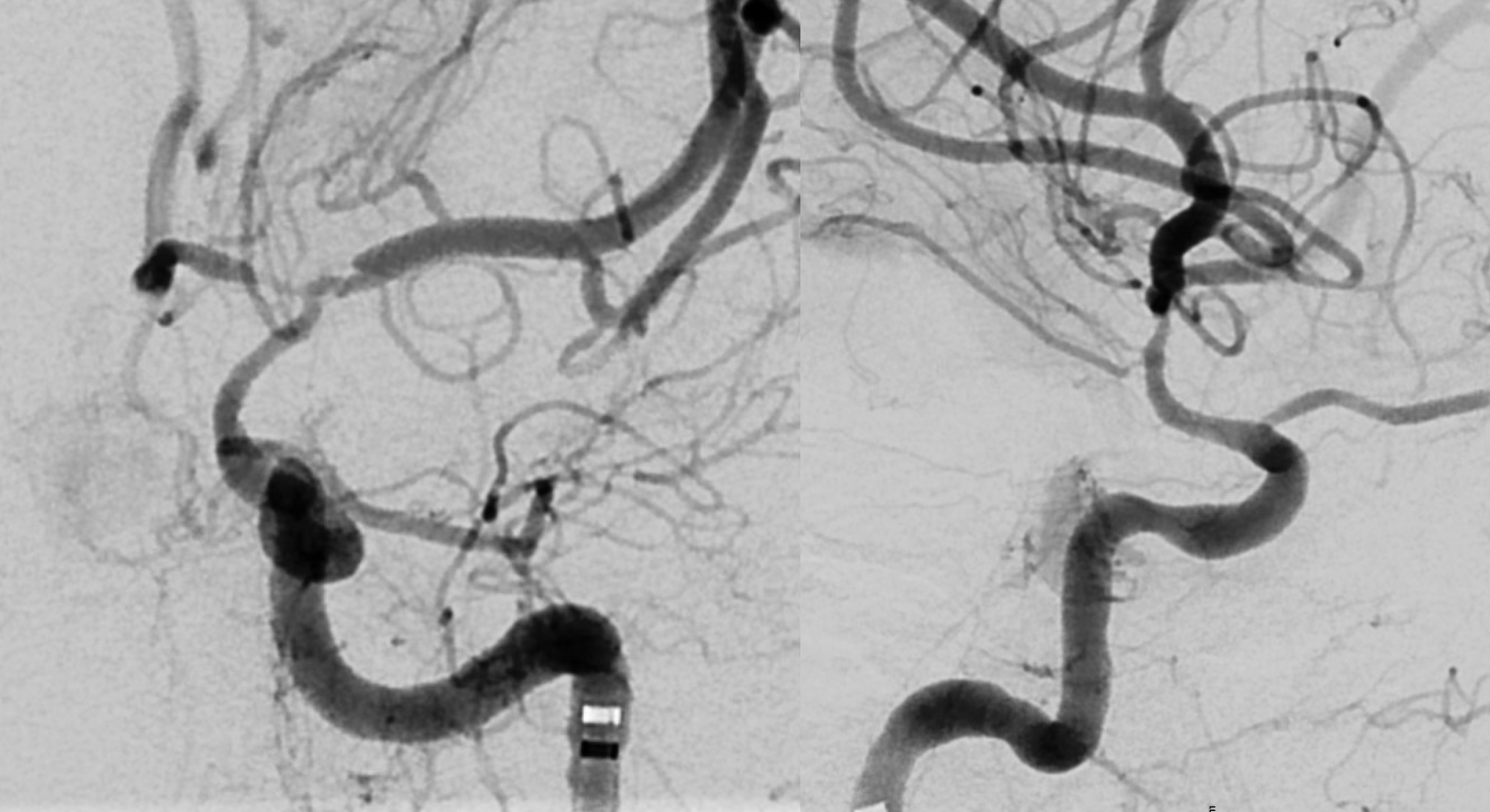
However, when “maximal medical management” fails with repeat infarcts, we are in SAMMPRIS territory. Here is a classic case of that, presenting with progressive supraclinoid/ M1 stenosis and repeat infarcts, while on everything medical
The major problem with SAMMPRIS stenting is perforator/side-branch occlusion. The main one here is the A1. Fortunately, that is well-supplied from the right side — and must be verified before going forward
Setup is BMX 80/SOFIA 5 ES 115/ Aristotle 14 standard 300/ Onyx Resolute 2×12
The major risk is anterior choroidal perforators. Notice that there are two vessels off the ICA — more proximal one is the true choroidal. The more distal is a choroidal-territory perforator that often originates from the ICA. It can original from choroidal as well. Sometimes there are more than 1 off the ICA. They are all eloquent. See anterior choroidal page for more info
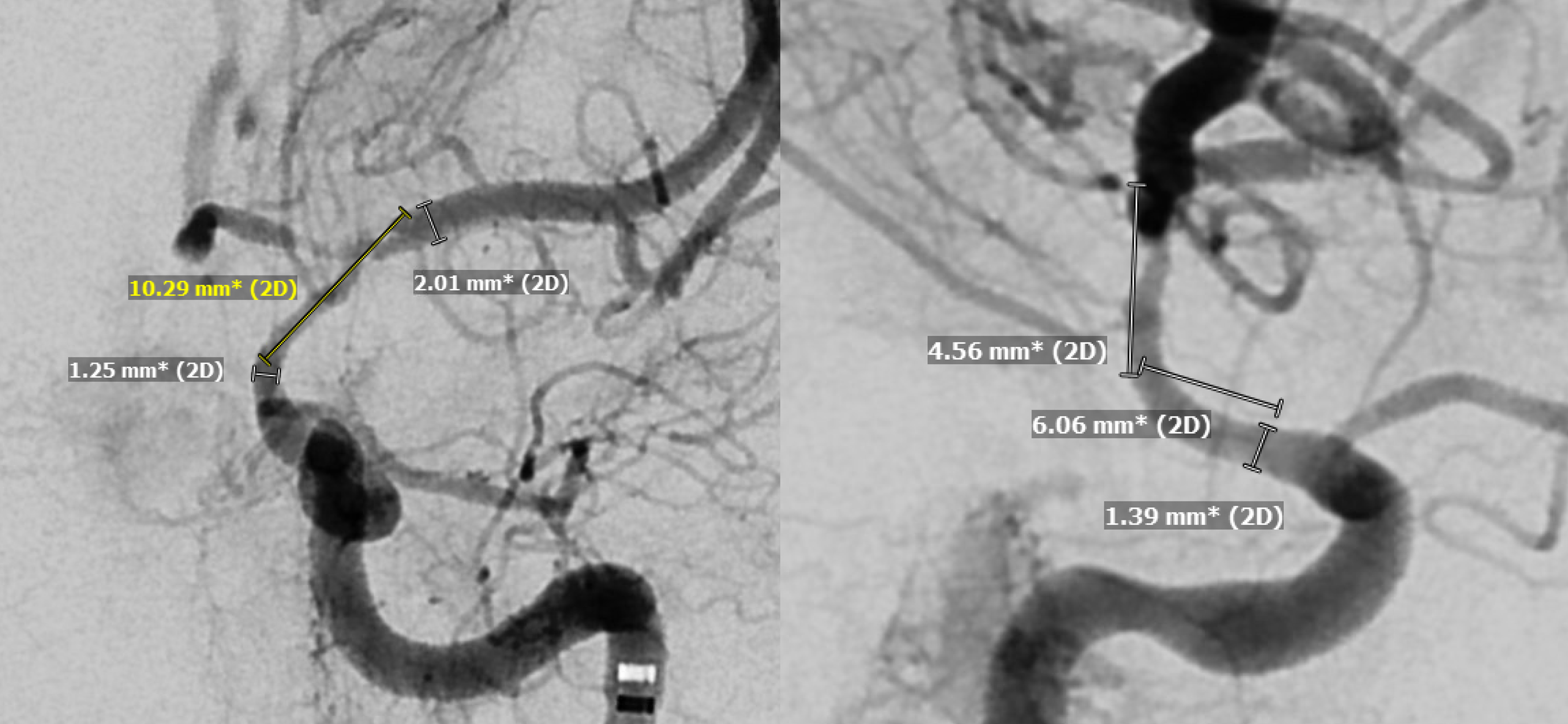
Measurements are what they are when balloon-mounted coronary stents are used. The length is a jump from 8 to 12 mm. We need a 10…
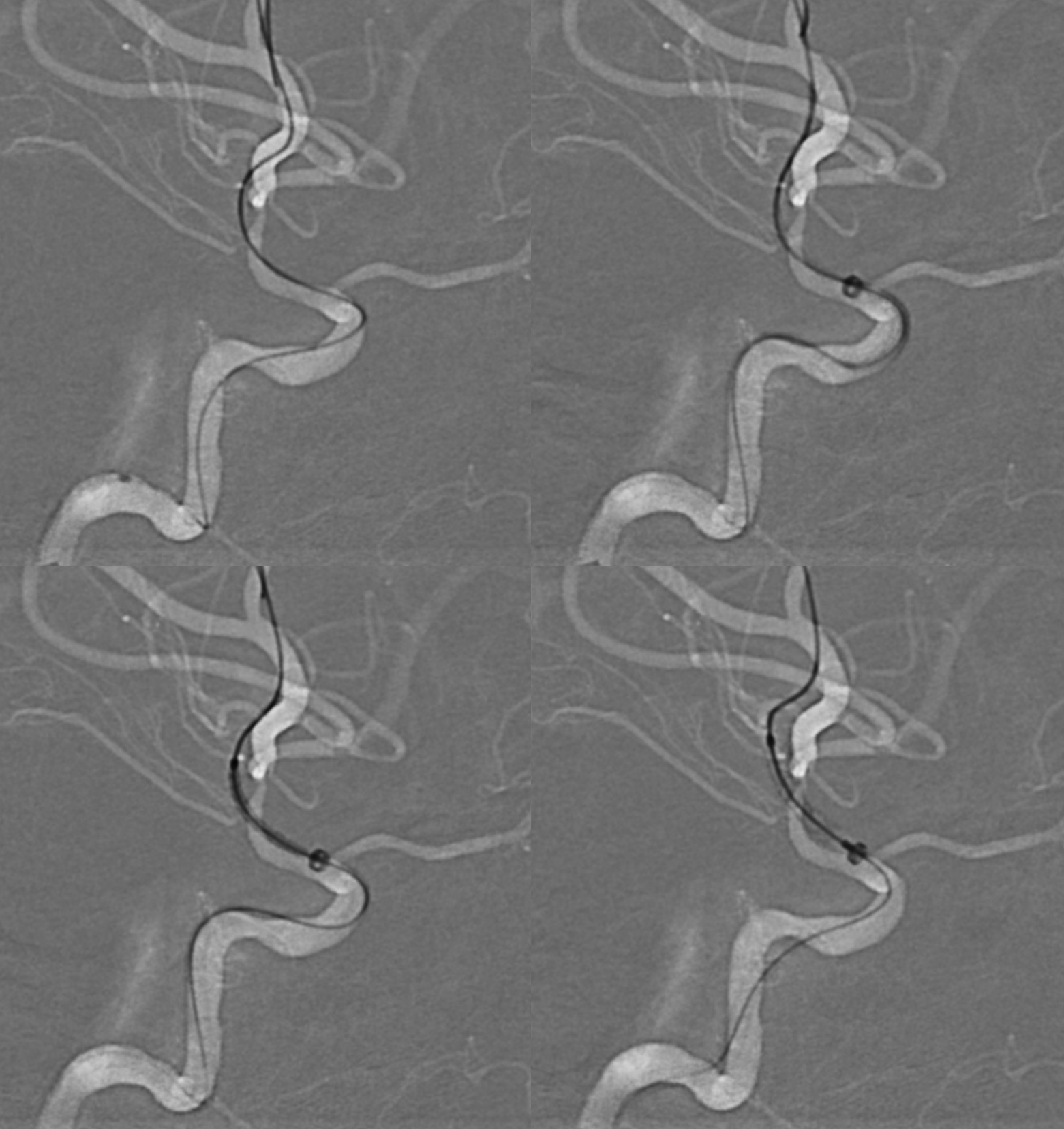
Stenting technique in our lab is standard — triaxial setup, good support. 1 — distal catheterization (J-wire helps with more support); 2 — bring up Sofia almost to the lesion; 3 — advance stent (Sofia helps a lot with that); 4 — deploy stent
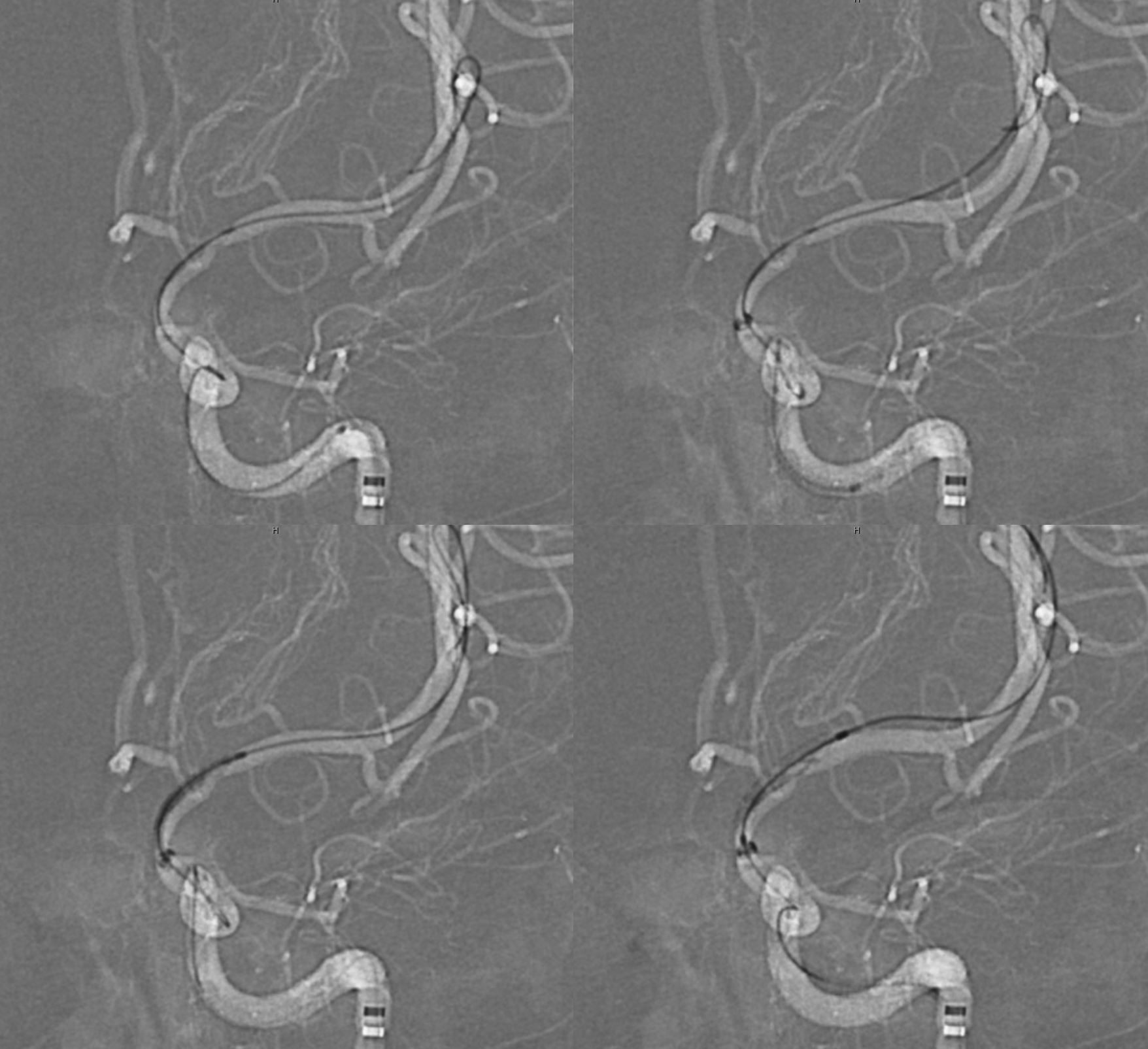
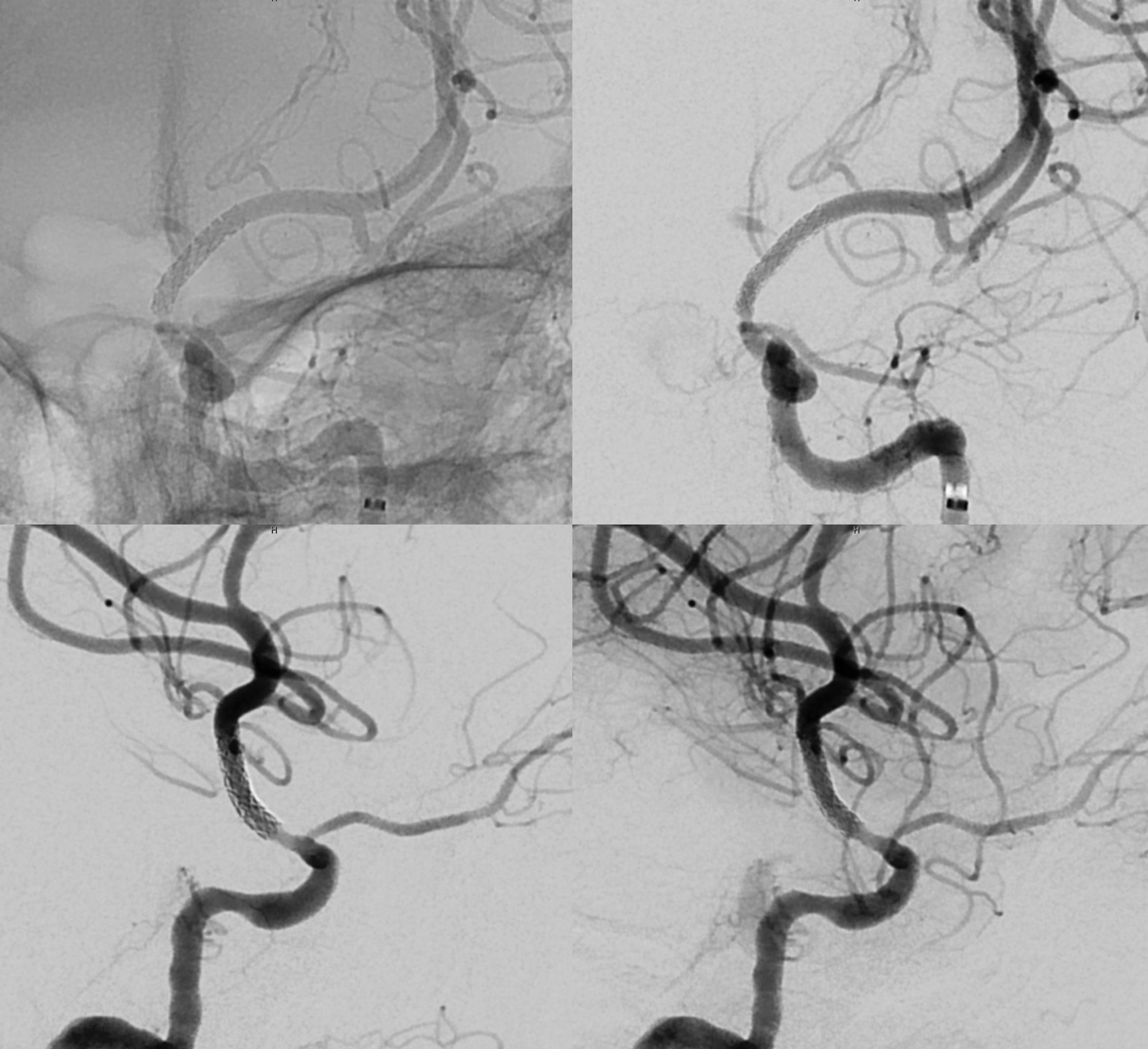
Post — notice something here?
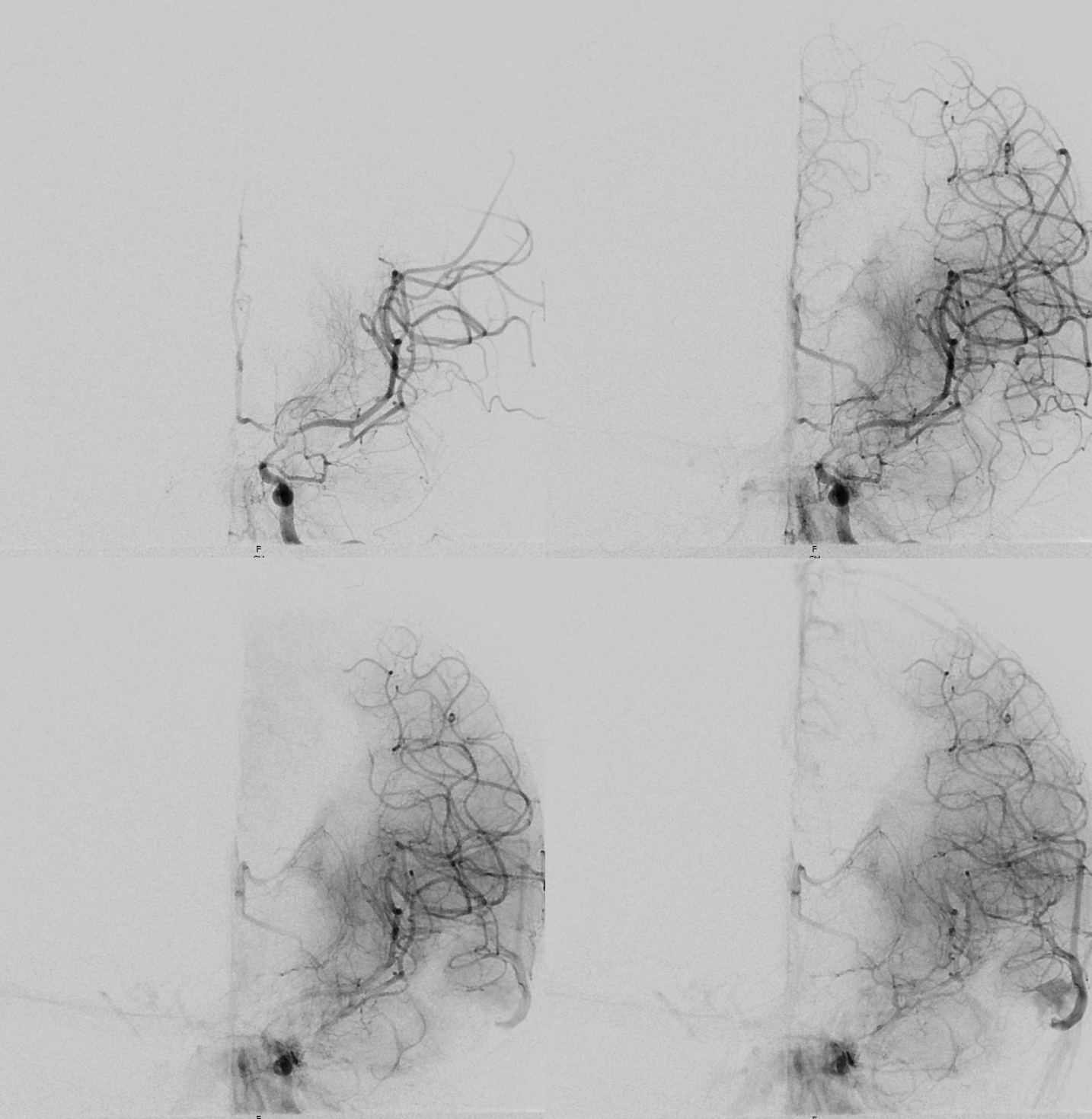
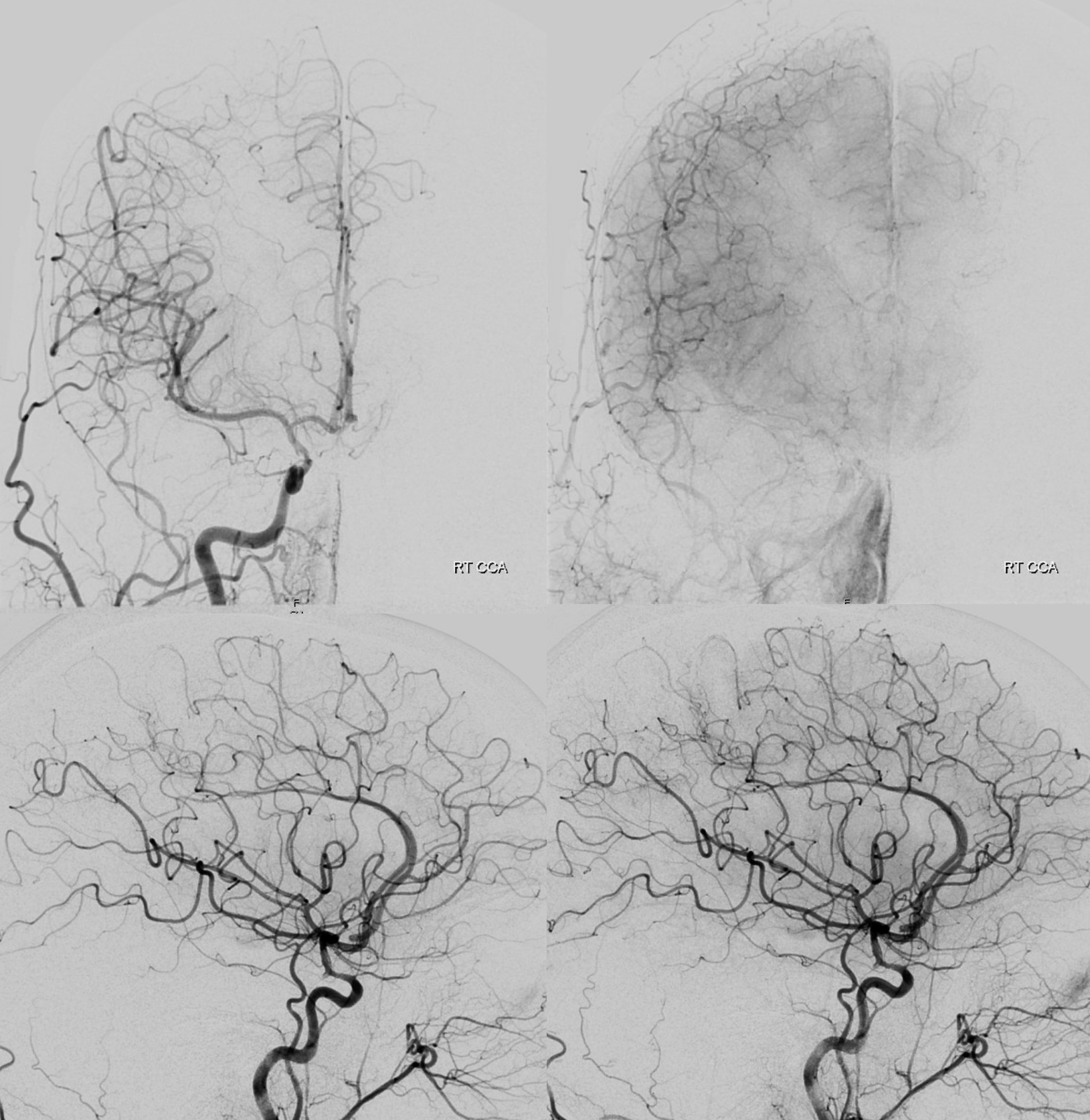
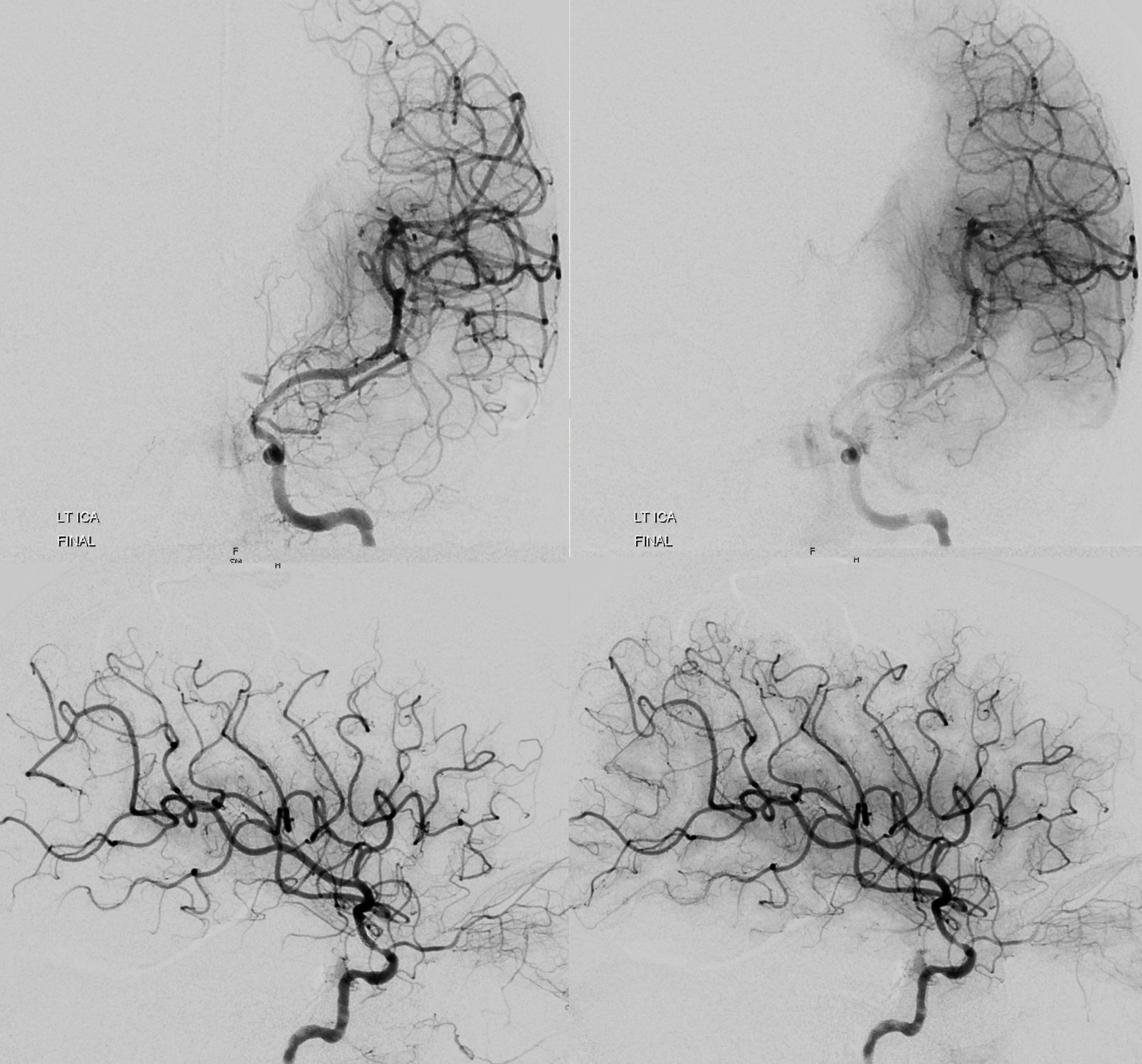
Global frontal and lateral — see something?
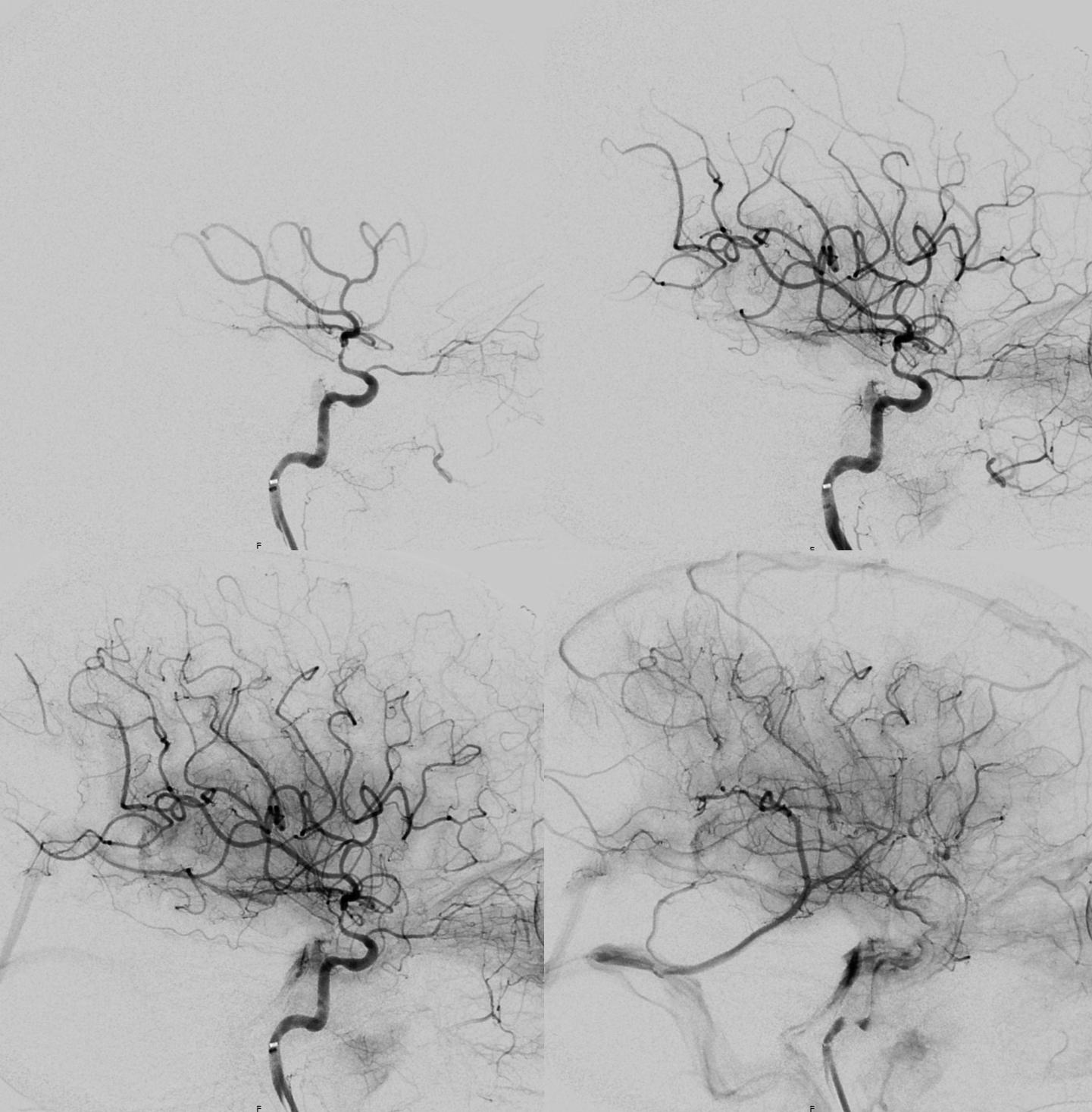
Post DYNA/VRT/MIP — see something?
What are the learning points relevant to SAMMPRIS? Aside from nicely opening the vessel, there are 3 areas where stenting changed something. There was no infarct — but there are 3 changes. What are they?
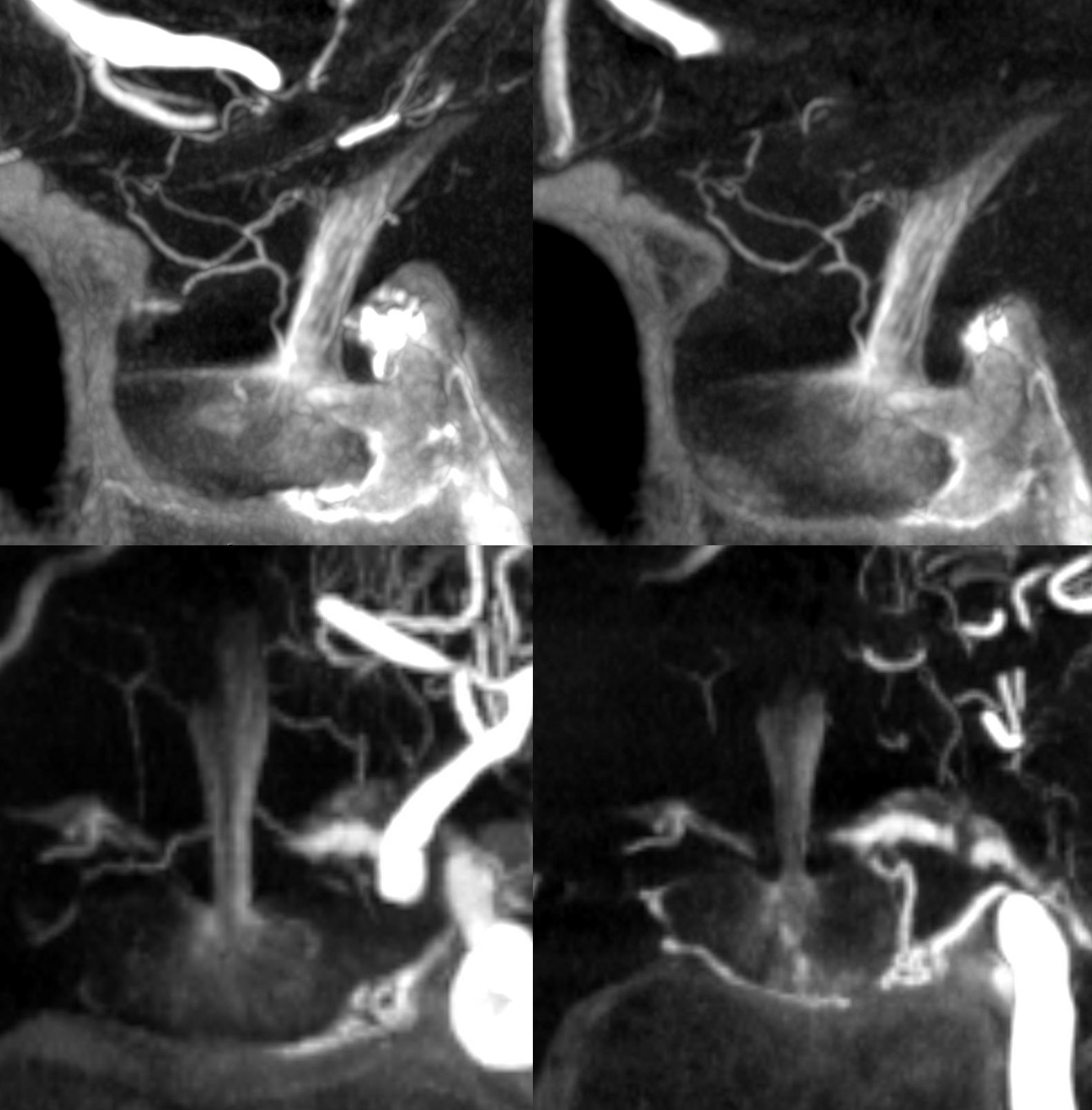
And, check out these beautiful pituitary images. The superior hypophyseal branches are occluded, presumably by athero. The posterior pituitary is supplied via the MHT. The anterior and stalk from the ACOM region