More tools means more options for MeVO and DVO. For aspiration especially, having an optimal diameter catheter is key. Its nearly impossible to measure that on CTA for M3 and M4, even M2 can be off if its smaller. The smaller the vessel the more uncertainty there is. We find it best to invest a minute into getting angiographic cross-sectional measurement — it will pay off handsomely if you get a good first pass
Presenation is with isolated severe expressive aphasia — the classic what-if for non-class 1A cases. Already on oral anticoagulation. There is a mid-M3 occlusion. This should be taken for thrombectomy. Video below
Or you can see images below
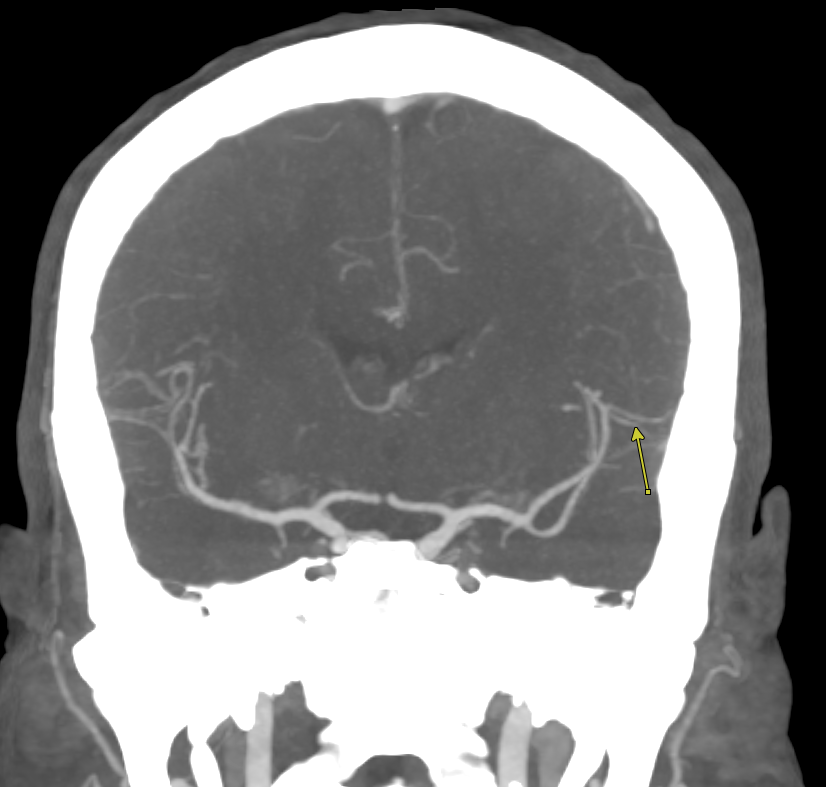
This measured 1.2 mm
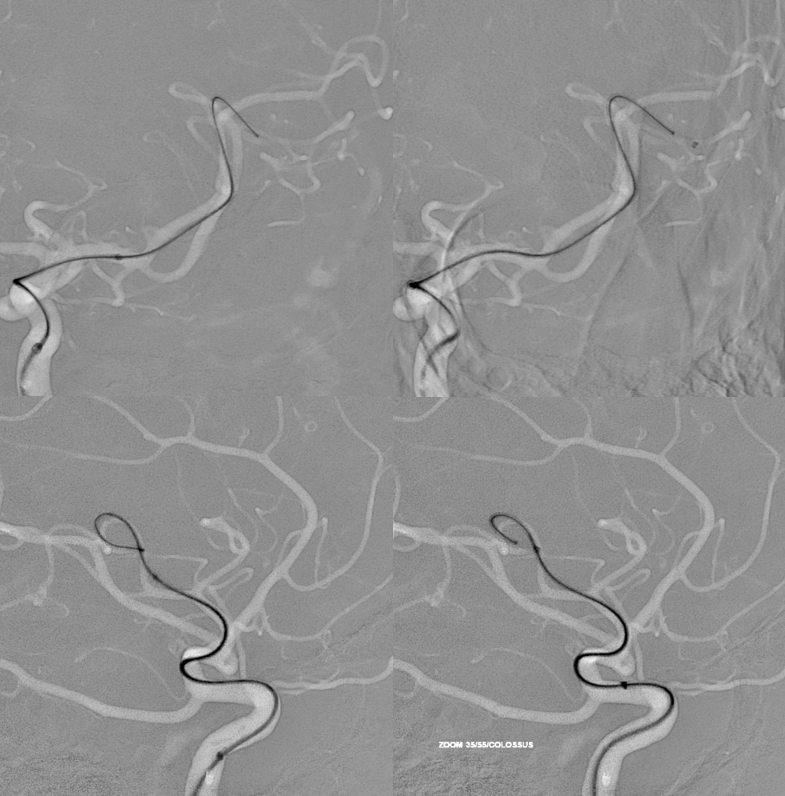
BMX 90 cm/Zoom 35/Zoom 55/ Aristotle Colossus. The 35 will go into 55 almost all the way — maybe 3-5 cm will not at the end — but that leaves at least another 10 cm with a y-connector. The Colossus 035 wire will usually fit into the zoom 35 — also only the distal portion is 035, rest is a metal wire of smaller diameter
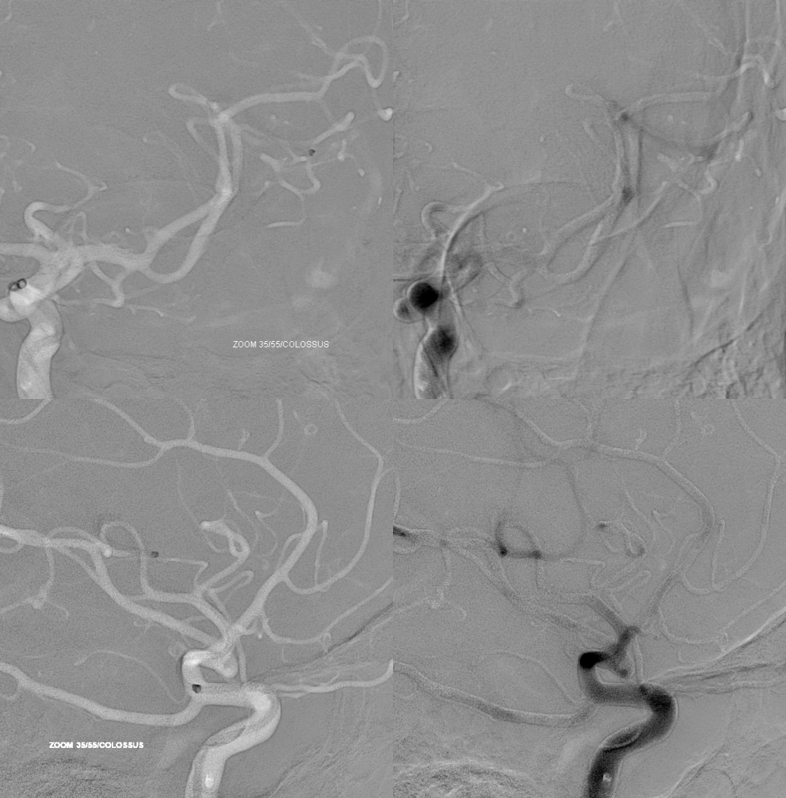
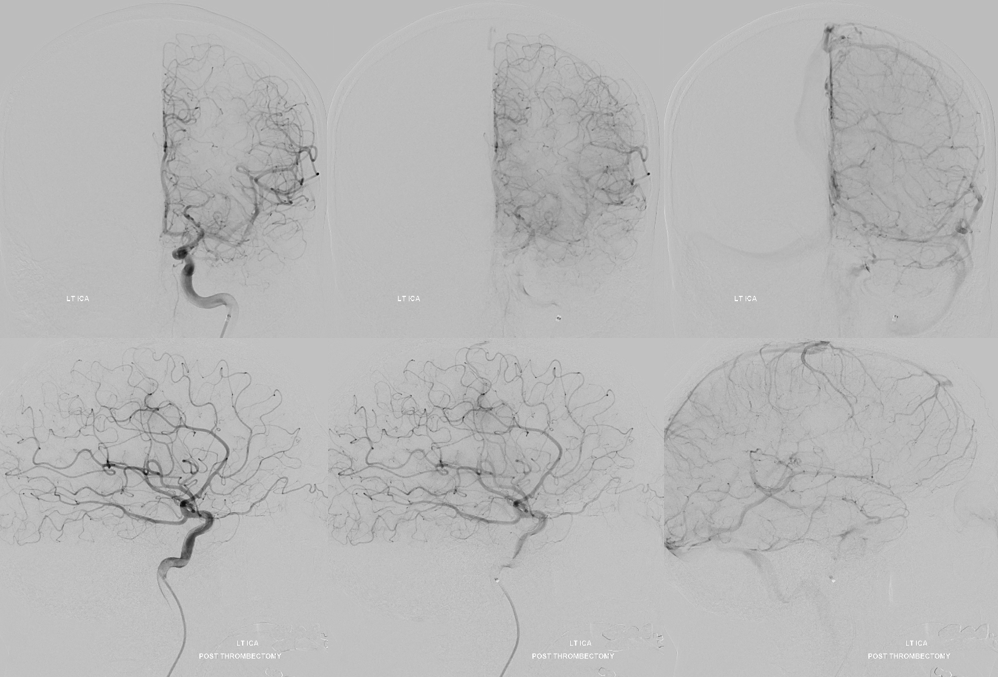
Post aspiration — two dark blue pieces of embolus were inside the 35
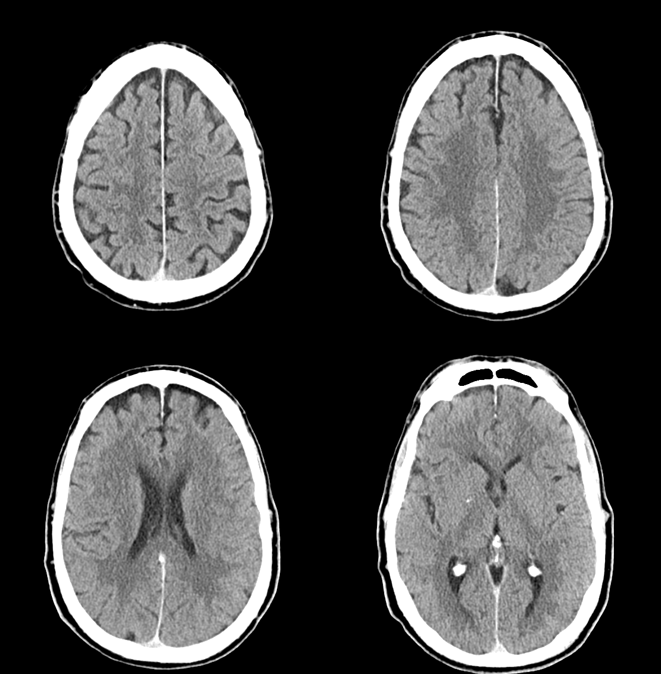
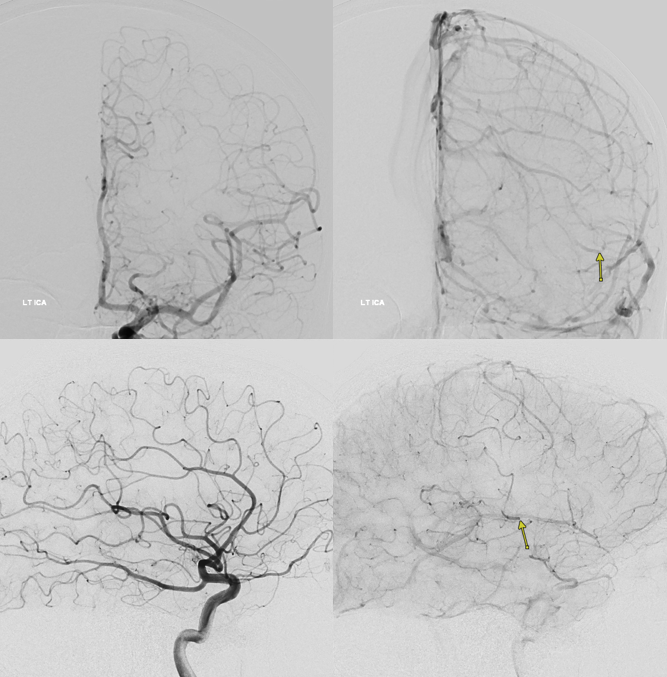
Note hyperemia and physiologic shunting in the reopened territory due to reactive vasodilatation — maximiming collateral perfusion. This is not a sign of dead brain — which also shows maximal vasodilatation. The difference is that living brain will stop the dilatation after a few minutes, while dead brain will not always do that.
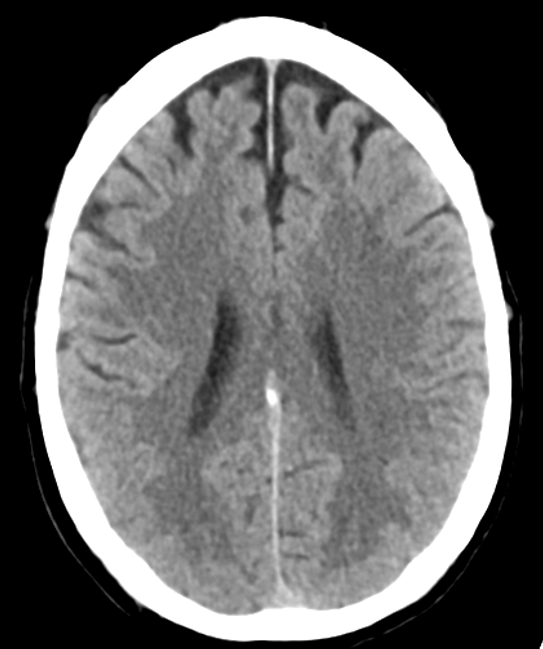
Post CT was normal. Exam normalized as well