
With Sara Rostanski and Eytan Raz
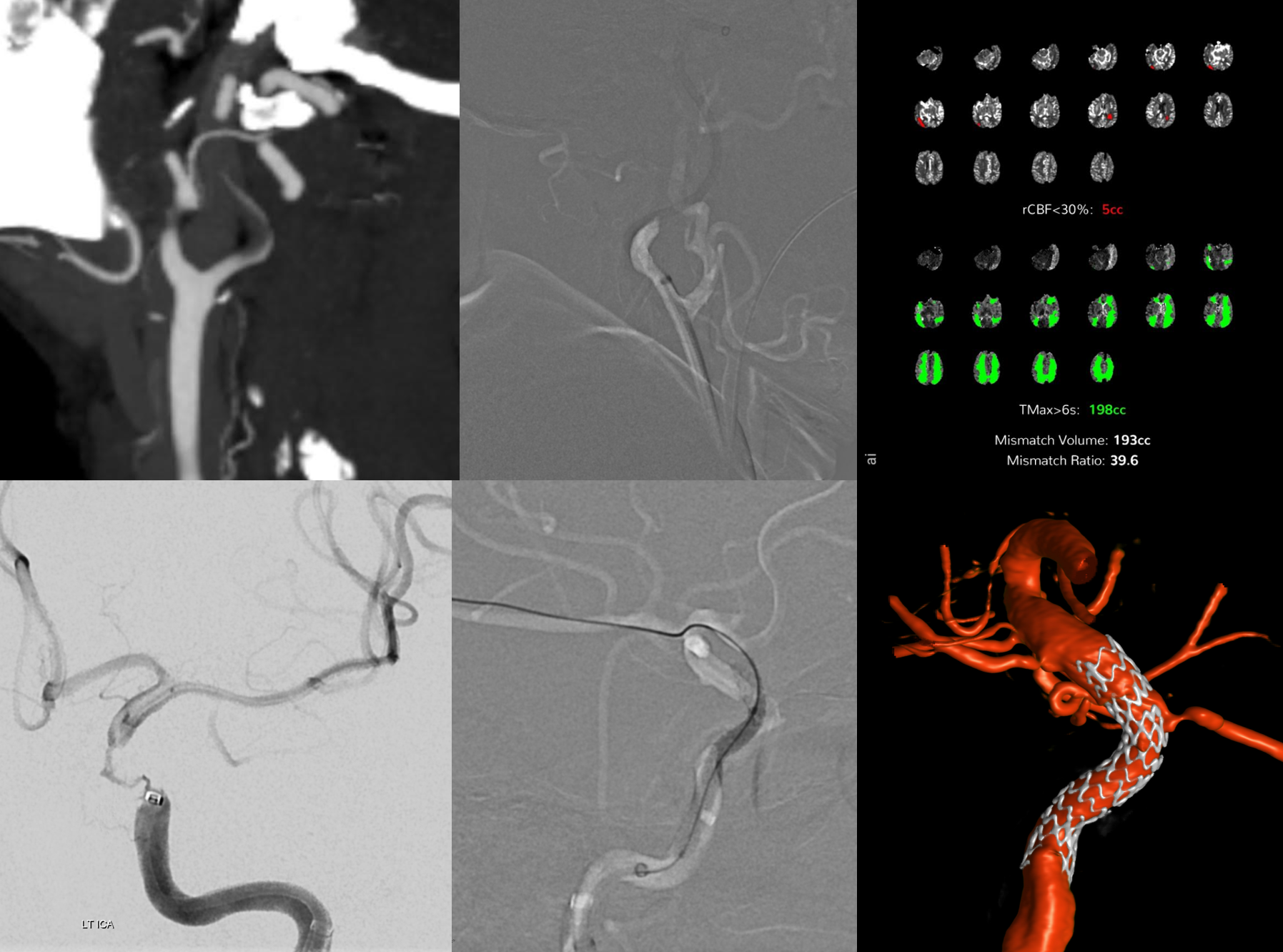
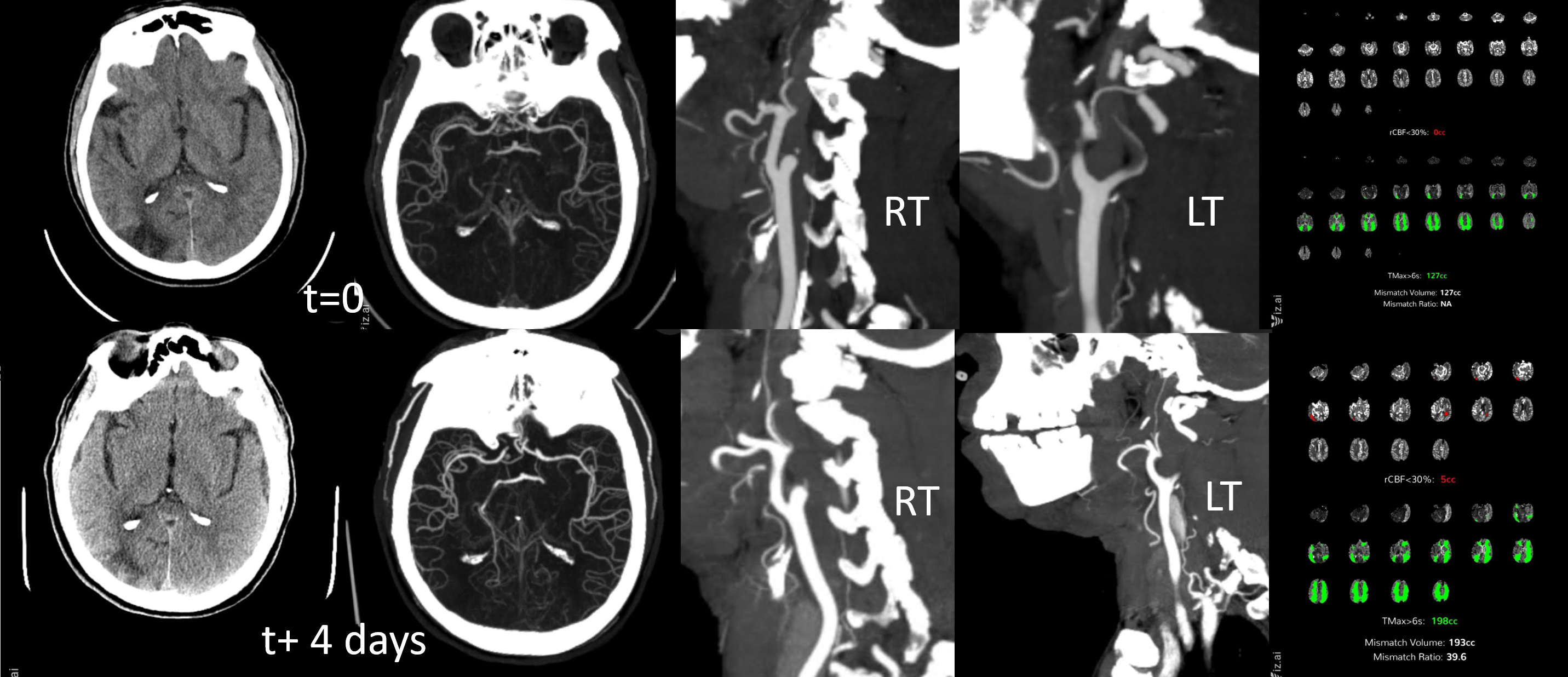
Subacute reopenings are not limited to embolectomies or cervical carotids. Any symptomatic occlusion that could benefit from reopening is a legitimate target. Here is a case of at least 4 days occlusion, initially with minimal focal findings, progressing to major focality. See below — the CT CTA CTP evaluation was repreated after deterioration. The right cervical carotid was chronically occluded. Left carotid was misinterpreted as chronic occlusion also. Notice however a obvious “flame sign” on sagittal CTA on day 0, which indicates a more cranial occlusion. On day 4 the flame sign is less obvious, due to progressive thrombus formation in the cervical carotid below the occlusion.
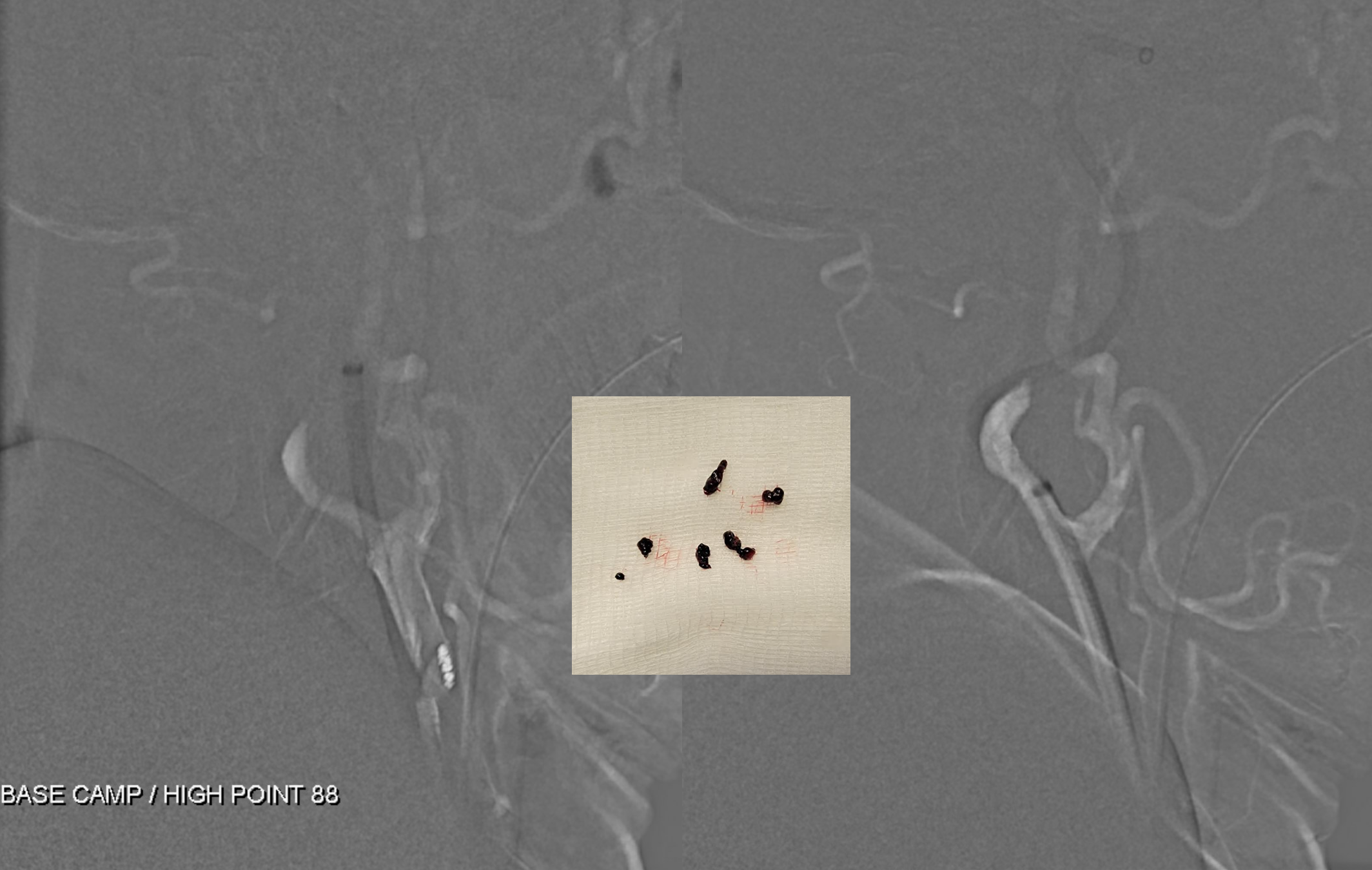
First job is to clear the cervical clot below occlusion. A Route 92 system is excellent for that. Base camp sheath (bare back femoral) and hi point 88
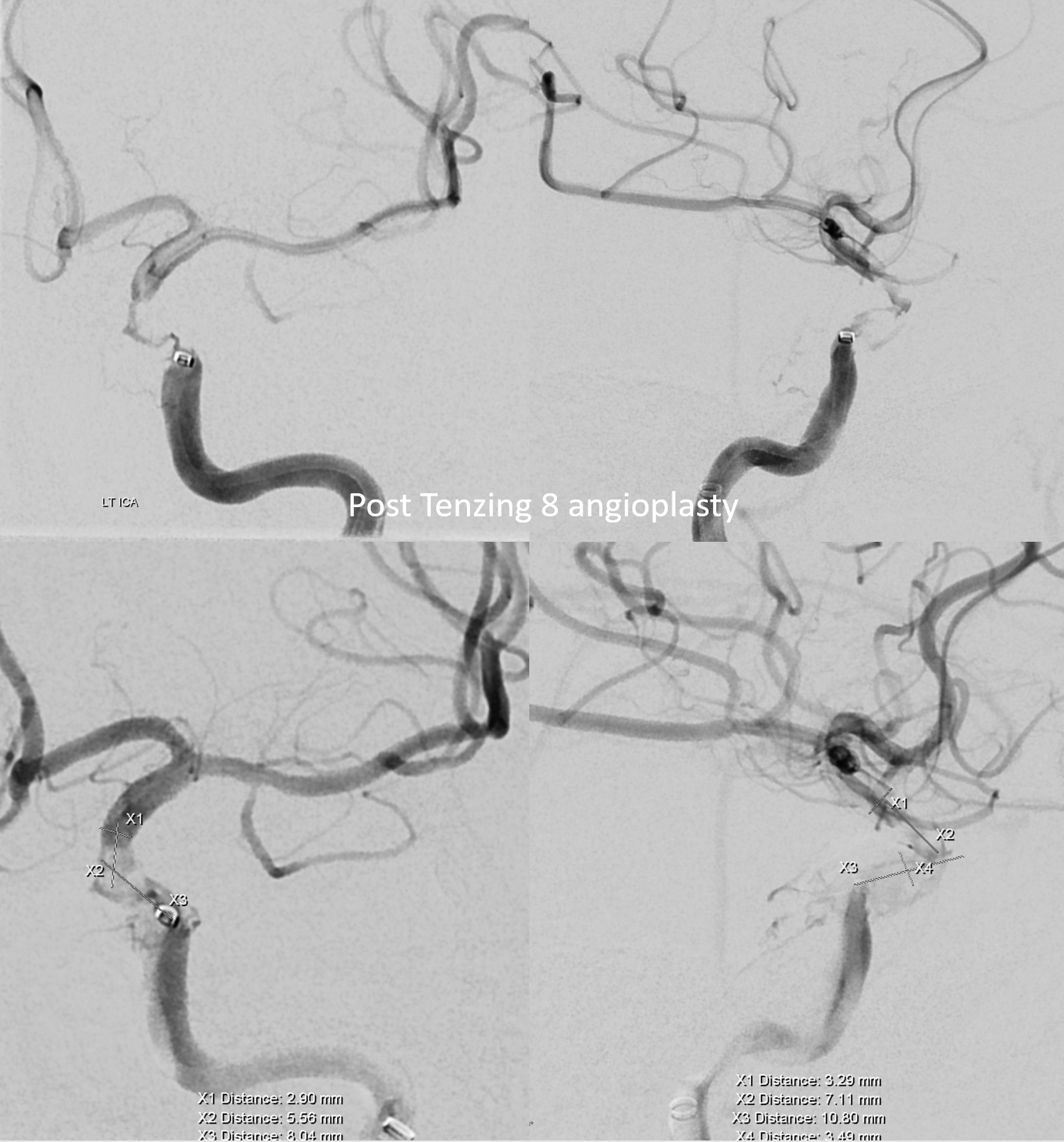
Combination of Tenzing 8 and Aristotle 14 was then used to go through the occlusion. unfortunately images not saved
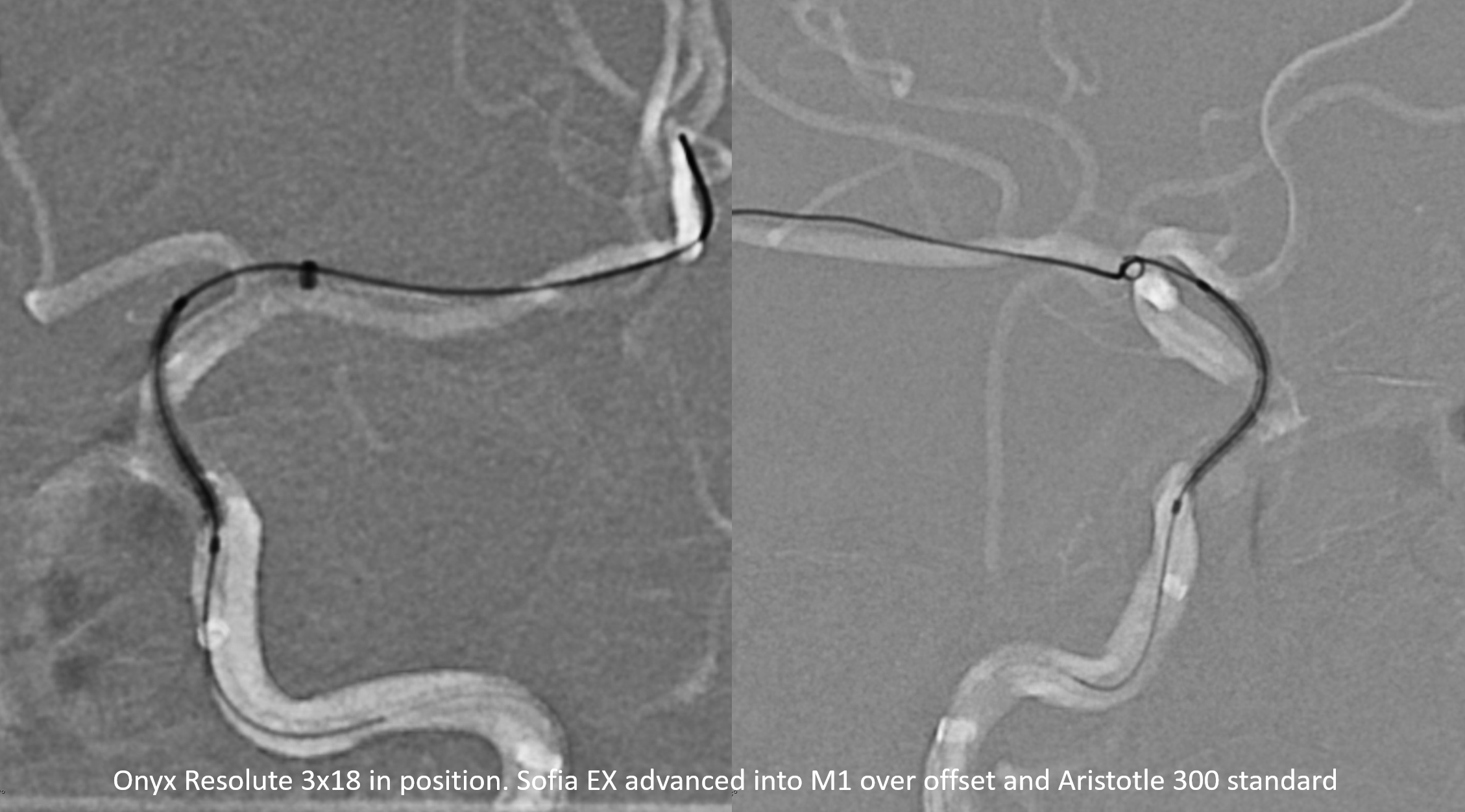
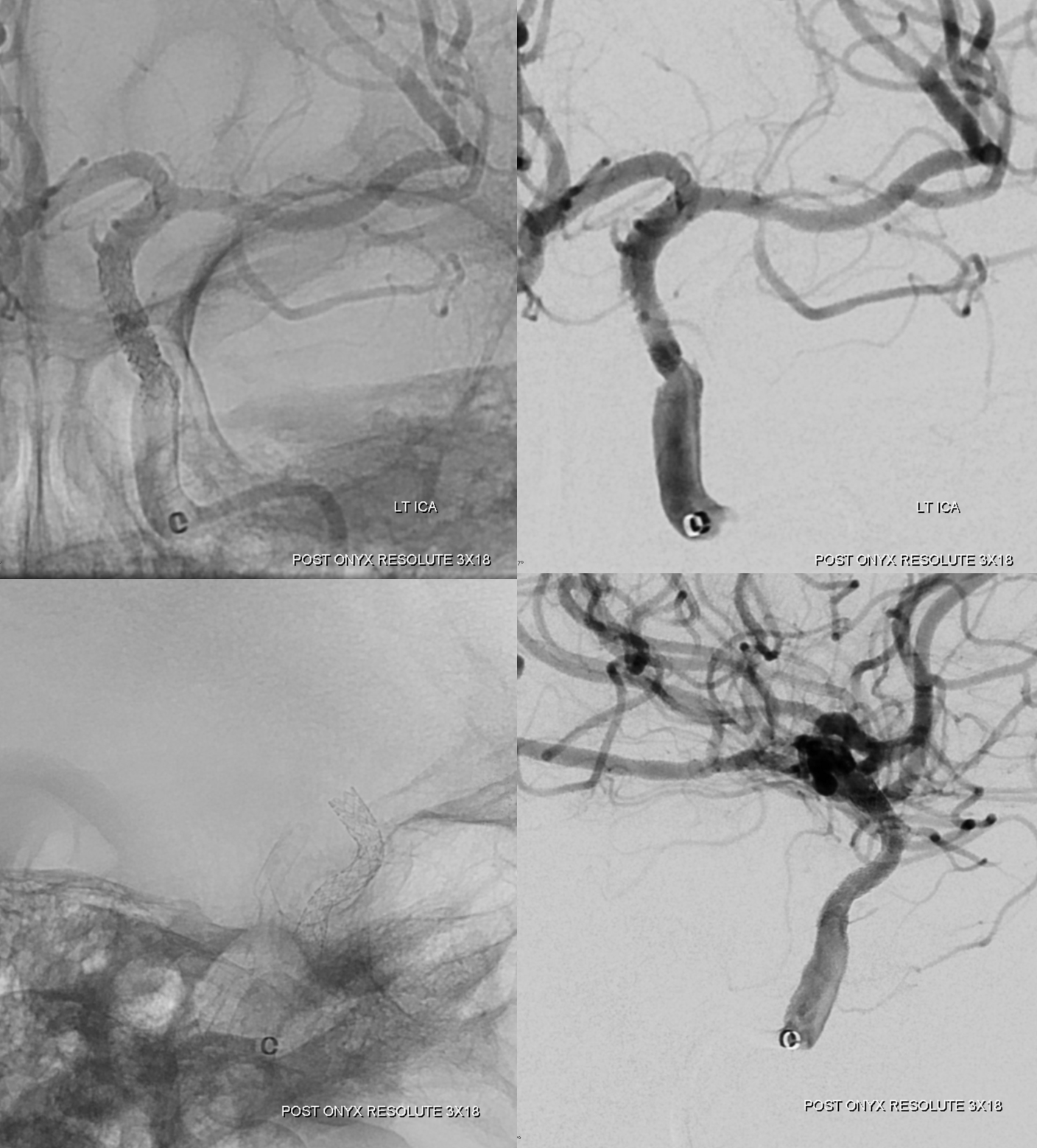
Here is one more key. Long stenosis needs long stent. Long stent is hard to push. Advancing intermediate past stenosis pretty much ensures it will work. Here, Sofia EX is advanced into the M1 over the Offset (a very underutilized tool, together with the wedge), and then the Onyx Resolute 3×18 is brought easily into position
Did a DSA to make sure we did not damage the vessel with major displacement
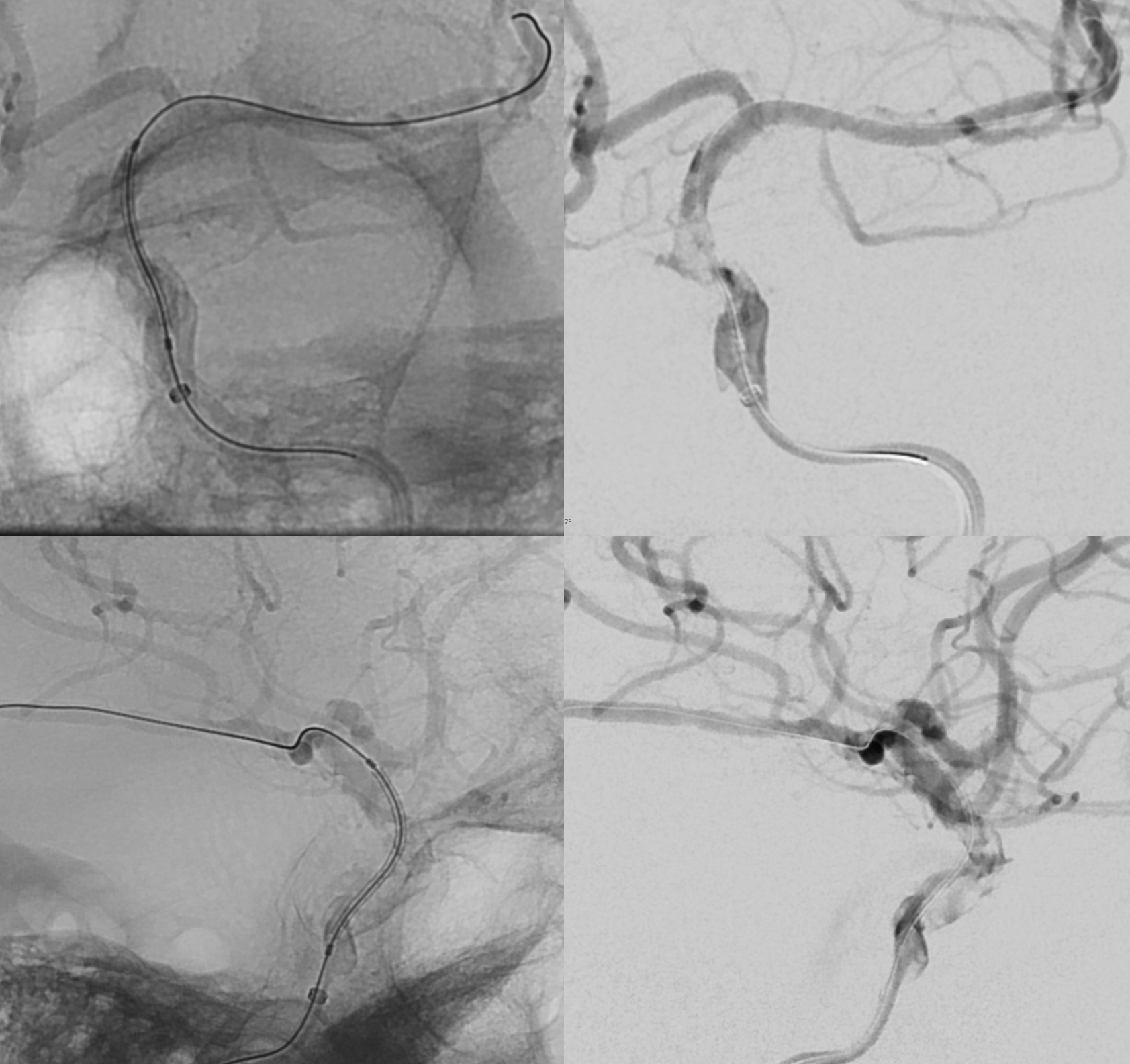
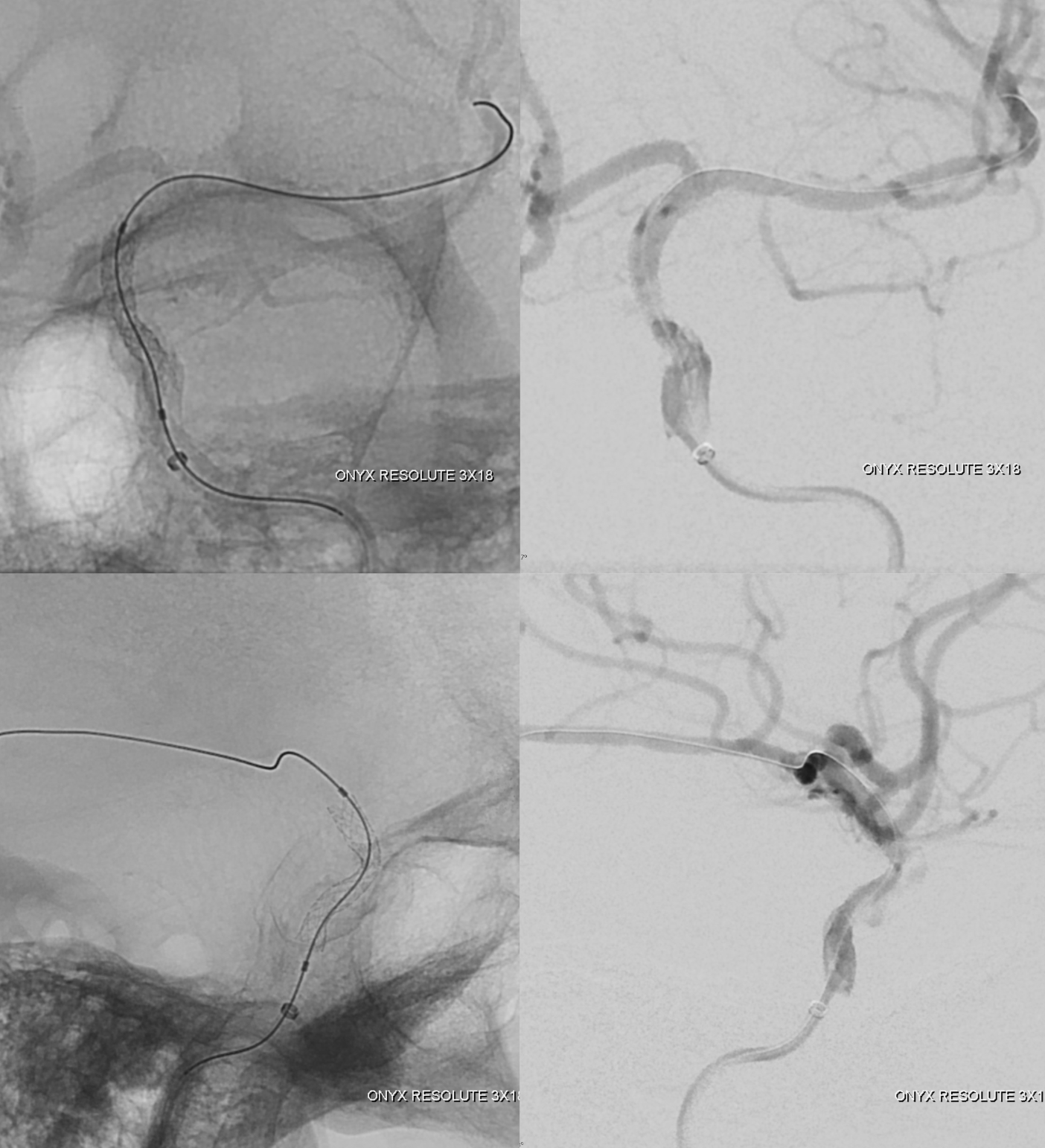
Deployment

no damage
We can inflate more selectively lower down
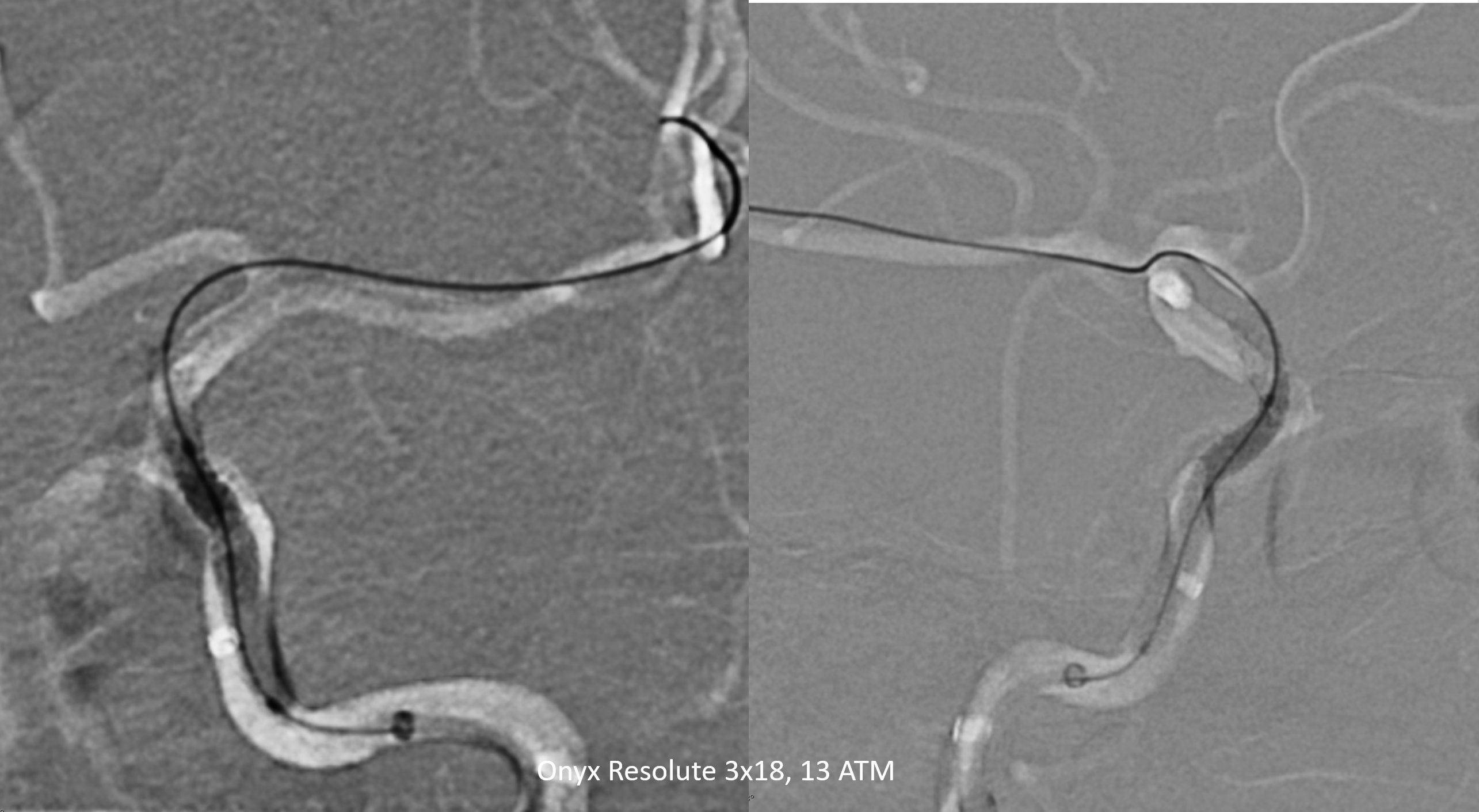
Post
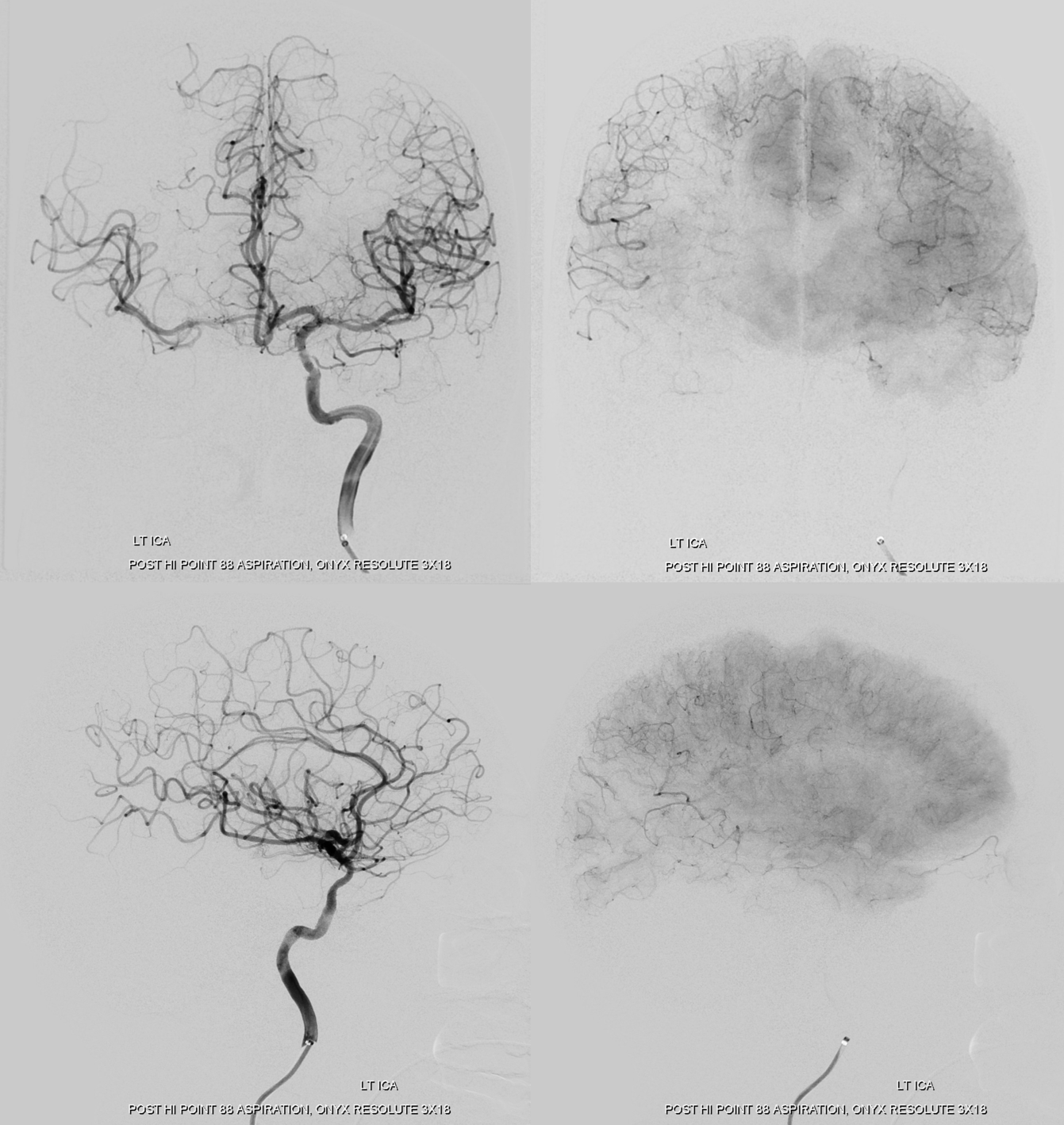
Right hemisphere is sitll starving some… Any ideas?
Final post save best for last — see how the relatively inflexible stent uplifts the supraclinoid carotid, with a shelf under the distal aspect. Nothing is perfect. if you make the stent more flexible, it will have less consistent radial force. Until we get something dedicated to the head (and it may not be better either), Onyx ones are still the best…
