
VEINS OF THE POSTERIOR FOSSA
INTRODUCTION
This is a particularly daunting topic, requiring much time and material, which delayed the development of this section until recently. The posterior fossa venous system is highly variable and consequently suffers from highly decentralized nomenclature. Its importance however is not diminished by these issues.
First, it is important to recognize that, angiographically, the posterior fossa veins can be visualized from both vertebral and carotid injections, and therefore full understanding requires some mental integration. To make things even more “interesting”, the entire posterior fossa venous system is seldom optimally visualized from a single vertebral artery injection — even when transient contrast reflux allows for opacification of the contralateral PICA, the amount of dye going into that system is not enough to provide adequate visualization of the corresponding venous territory. Therefore, if there is particular clinical need to understand posterior fossa venous structures, it is probably best to inject both vertebral arteries. Examples of this are provided below.
Fundamentally, I think it is very useful, particularly in learning stages, to forego semantics in favor of anatomical localization. The nomenclature, beyond the most fundamental veins, quickly becomes divergent and confusing. These frustrating issues nevertheless serve to highlight the fundamental and reassuring truth, that it is less important to name the vein as to know where it is and, therefore, what brain structures lay next to and are drained by it. The key here is to understand the location of the brainstem relative to the venous structures. Nothing is more important in understanding posterior fossa veins. This can be difficult to conceive, but once you have the brainstem down, lots of other things fall into place as well. To this end, several strategies can be employed. One is to study veins on MRI — T2, CISS, PRESS, post-contrast volumetric gradient echo T1 (such as MP-RAGE) — are often much easier to understand than catheter angiographic runs, though only the larger veins can be seen. Another approach is to look at the arteries first, and deduce the relationships from there. You can scroll through the angiographic run, or step through the mask to allow the arterial phase to serve as the mask for the venous phase, visualizing both entities simultaneously. Also, it is helpful to study CTA sagittal MIP images to have a mental picture of how position of the brainstem is related to the osseous structures of the calvarium (it is variable, of course, but still very helpful).
Finally, having the ability to view things in stereo is a big advantage. The experts certainly need it less, but personally I find that the degree of insight is substantially augmented by stereoscopy in both AP and lateral planes. Some of my colleagues have bought dedicated prism glasses to be able to stereo without having to cross their eyes — the basic models are quite affordable and may be worth it if you are not having luck with eye crossing. Even so, about 10% of the population cannot view in stereo (for eye crossing, at least). While this may seem like a disadvantage, I imagine that with persistence one will achieve the same degree of understanding as stereo-capable colleagues, while reaping the benefits of reduced dependence on ancillary techniques.
Finally, and perhaps most importantly, for all of us, there is no substitute for time investment. The more you stare at / look for these veins, the more you’ll know.
OK, now to the important parts — pictures.
GENERAL ASPECTS OF POSTERIOR FOSSA VENOUS ANATOMY
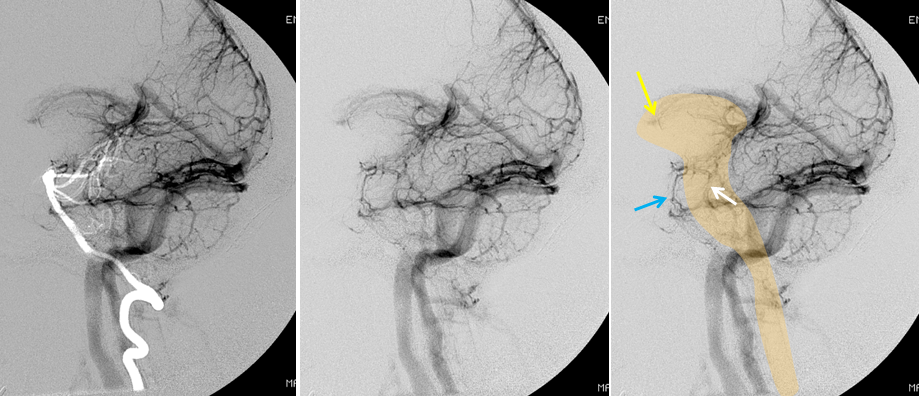
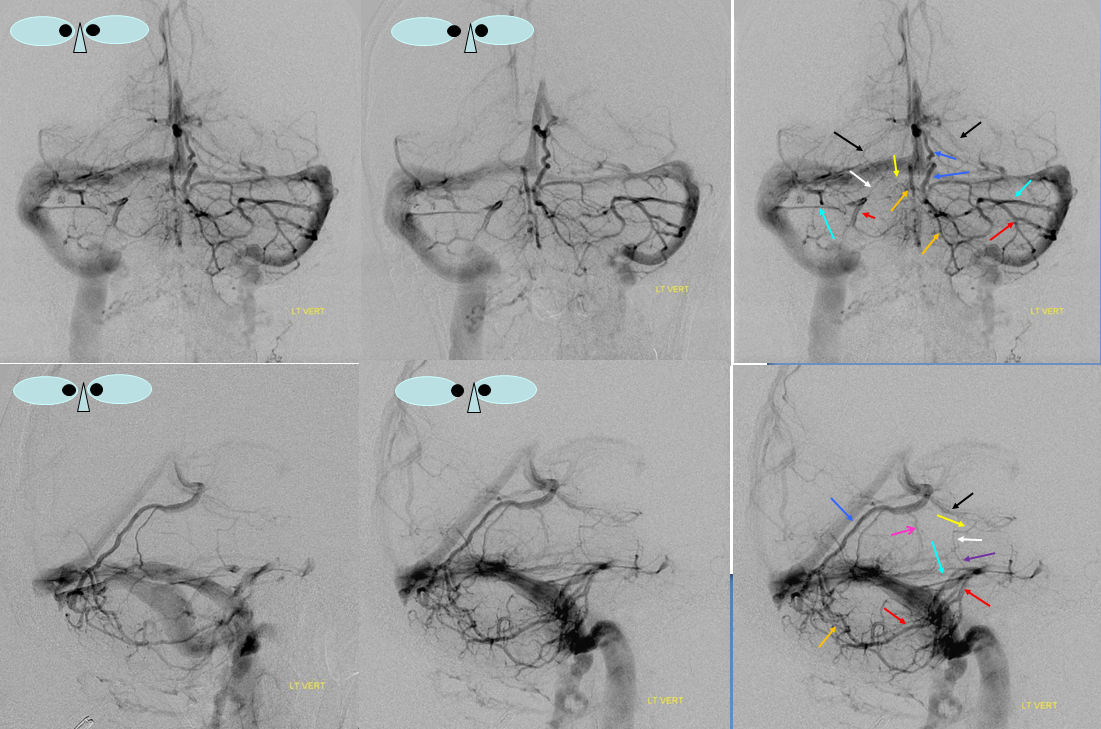
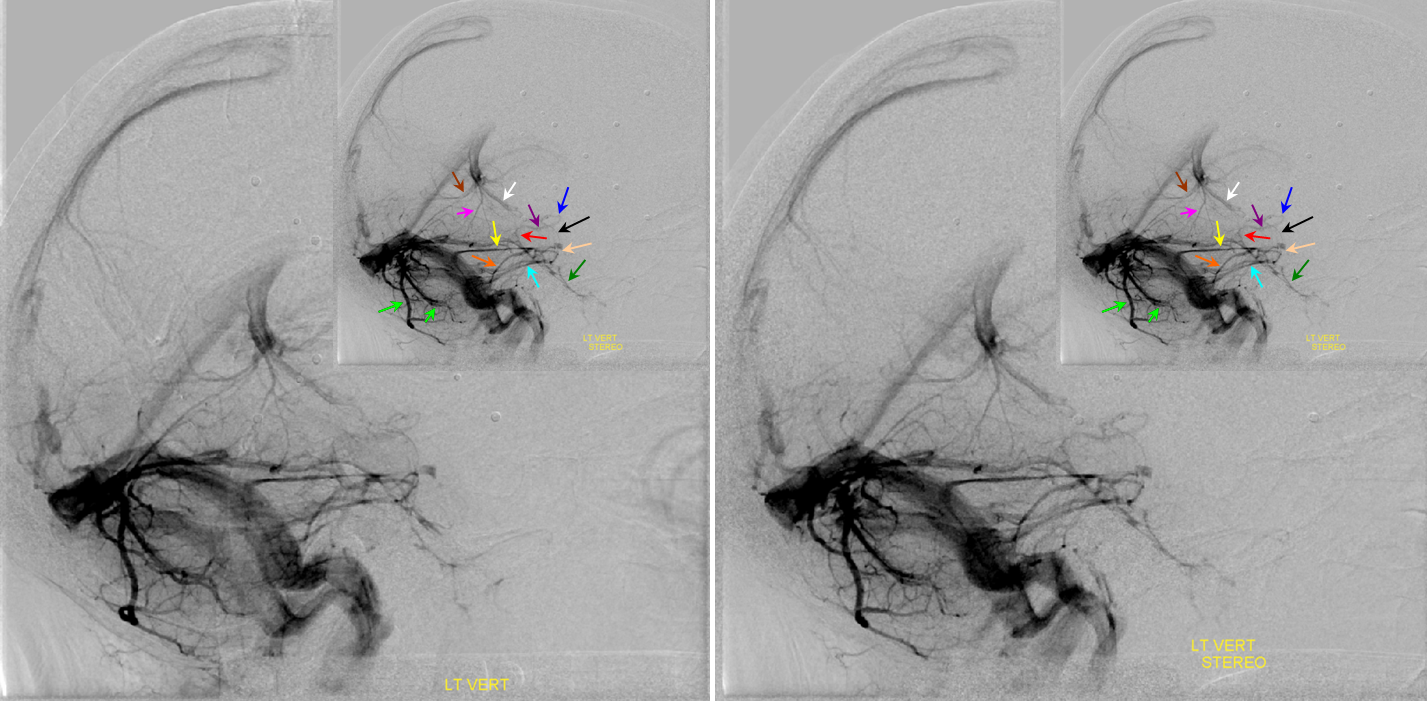
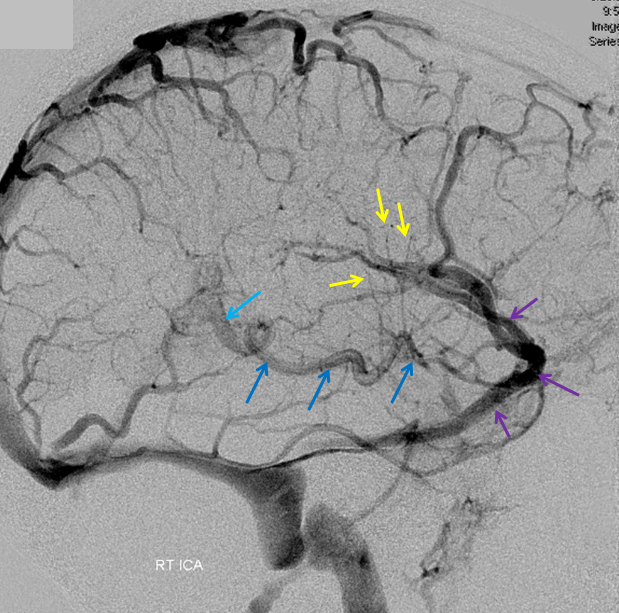
A series of lateral angiographic venous phase images. The image to the left is made by adopting the arterial phase of the same injection to serve as the mask image for the venous phase. This helps establish important relationships in terms of the location of the veins reltaive to the brainstem, which is superimposed on the right image. The arterial mask image, for example, helps appreciate that the large vein denoted by the blue arrow is a prominent anterior pontomesencephalic vein (which is located anteriorly along the basilar artery), and not the more posteriorly located lateral mesencephaic vein (white arrow). The foramen of Monro is almost always going to be close to the anterior most aspect of the lateral choroidal vein (yellow arrow)
Angiographic Projections
Generally, the Townes or an even more steep craniocaudal view is a good idea for visualizing the posterior fossa veins. It has the advantages of elongating the basal vein, and projecting the brainstem structures inferior to the torcula / transverse sinuses, and therefore without undue superimposition. AP or Caldwell views may be good for some aspects — for example, in the Townes view both superior and inferior cerebellar surface veins will project below the transverse sinus — the lateral projection helps in this case, and a Caldwell or AP can be good too. Generally, though, Townes or another steep craniocaudal view is best. For example, while Caldwell is very good for looking at the basilar artery, it does not work well for the anterior pontomesencephalic vein, which is too small and gets lost in the overlying shuffle. In the lateral projection, a somewhat oblique (along the craniocaudal axis) view will separate the left and right homologous structures, which would otherwise be superimposed.
Importance of understanding limitations of angiographic injections
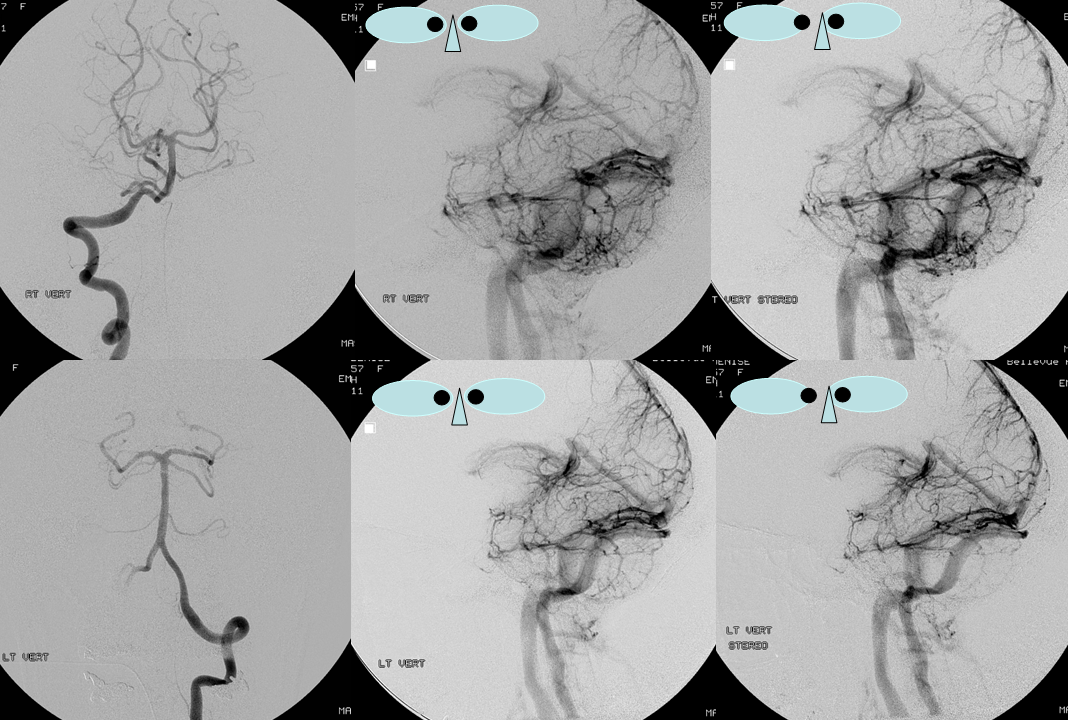
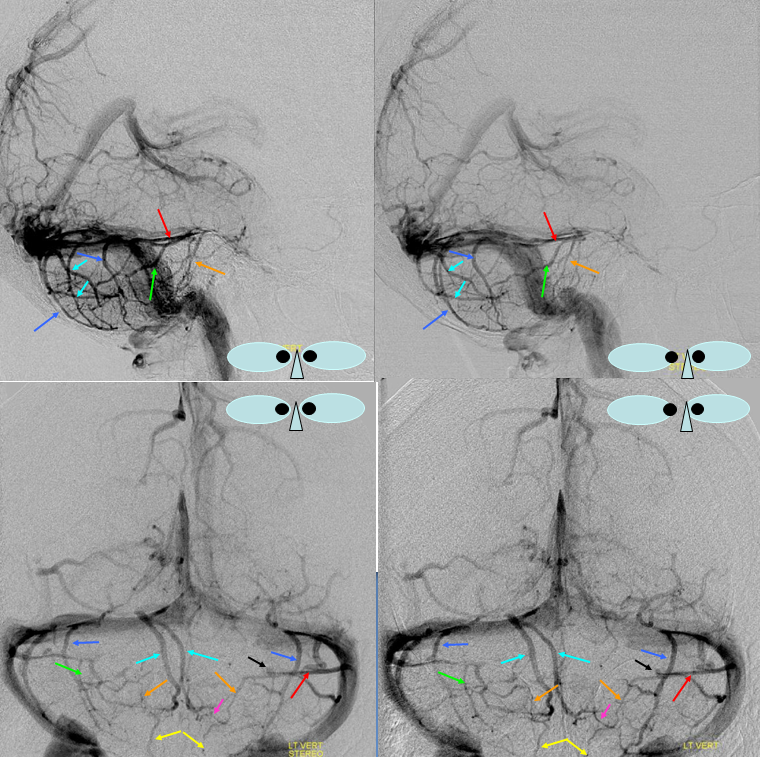
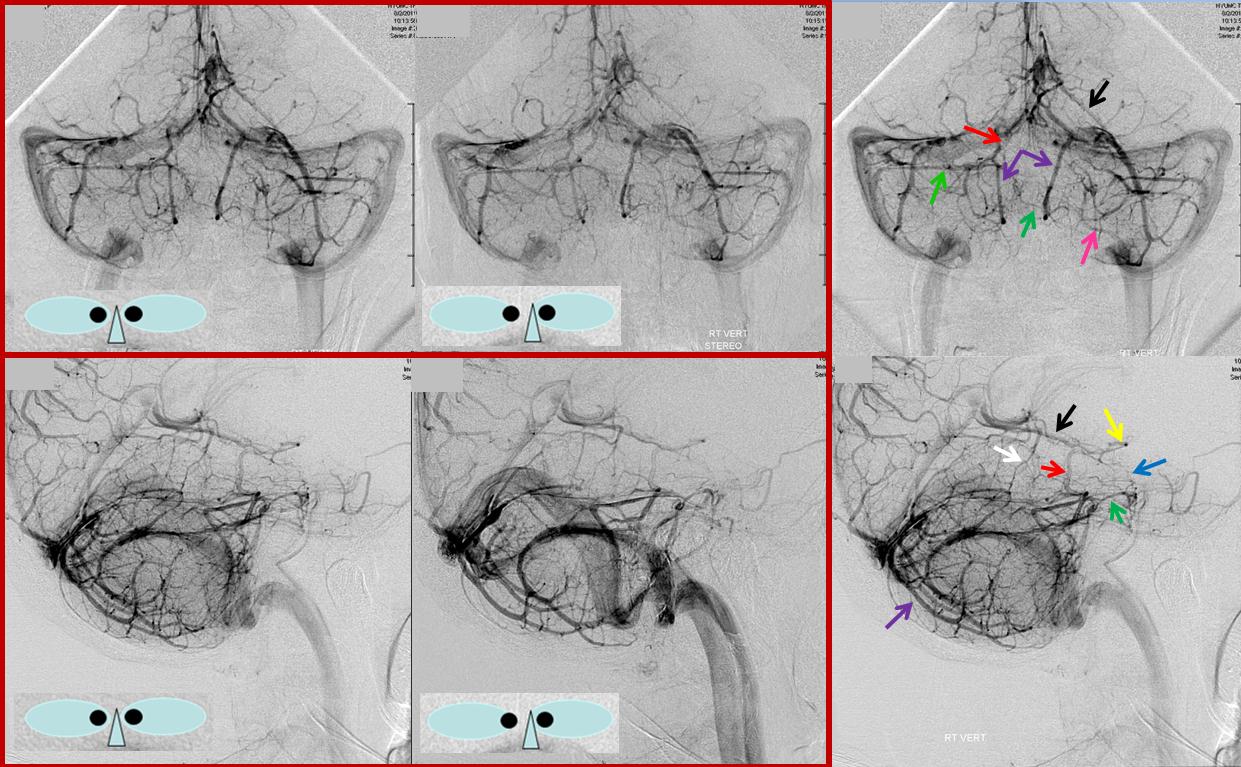
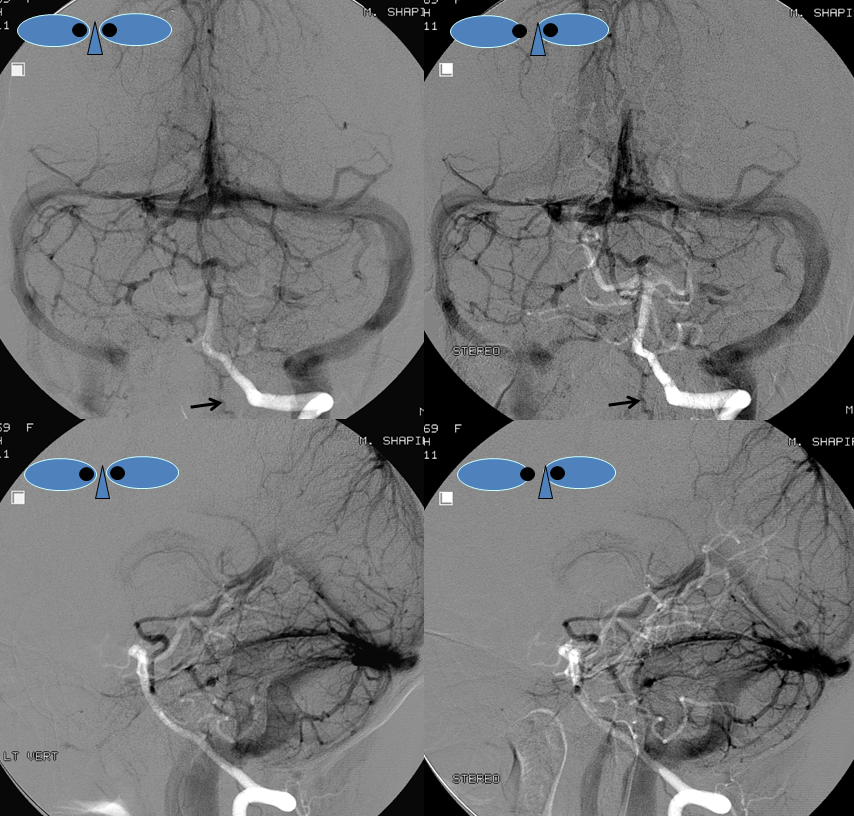
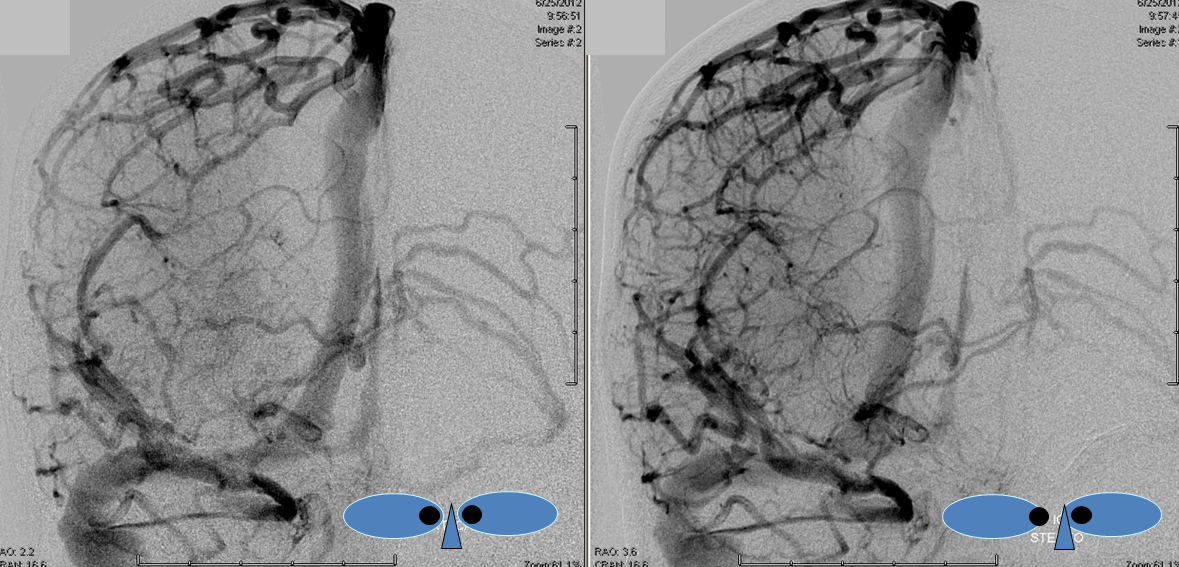
Angiographically, you can only visualize the veins of a corresponding arterial territory. It is very important not to forget this. The top set of images show lateral stereo images of a right vert injection, which opacifies a dominant right PICA. The bottom row of left vertebral artery images, from the same patient, shows markedly poorer visualization of the cerebellar veins. Even though right PICA was transiently opacified (bottom left AP image), the amount of contrast delivered into the right PICA (which supplies so much of the cerebellum) is not sufficient to produce adequate venous filling.
Brainstem vs. cerebellum
It can be helpful to separate, albeit artificially, the venous apparatus of the cerebellum from that of the brainstem. Here, we’ll examine the cerebellum separately from brainstem structures, keeping in mind that anatomic variation is the mainstay in drainage of both structures.
Cerebellum
The three-surface concept of the cerebellum is very helpful in understanding its venous drainage. Basically, you can conceptualize each cerebellar hemisphere as a geometric structure with three surfaces — posterosuperior, posteroinferior, and anterior. The posterosuperior surface is the top, underneath the tentorium. The posteroinferior is the back and lower surface, and anterior is what’s facing the brainstem. In the vertical plane between the two lobes sits the C-shaped vermis.
The veins are located on the surface of the cerebellar hemispheres, and generally drain into the adjacent sigmoid and transverse sinuses, with the exception of the vermian veins. The course of the vein, and its point of connection with the sinus help identify the surface it is running along. For example, the veins coming up from below the transverse sinus and entering the more proximal (with respect to the torcula) aspect of the sinus must be located on the mesial posterior surface, whereas a similar vein below the transverse sinus and draining into its distal aspect has to be located on the lateral aspect of the inferior surface. Veins draining into the superior or inferior petrosal sinuses must, at some point, run on the anterior surface, since the petrosal sinus is located anterior to the cerebellum. In the midline, along the vermis, run the superior and inferior vermian veins.
Usually, you will see that for each hemisphere, one of the three surface veins will be dominant, — for example, a large inferior surface vein and smaller superior and anterior surface veins will be present. The same goes for the vermian veins. And even more so for veins of the brainstem (dedicated treatment below)
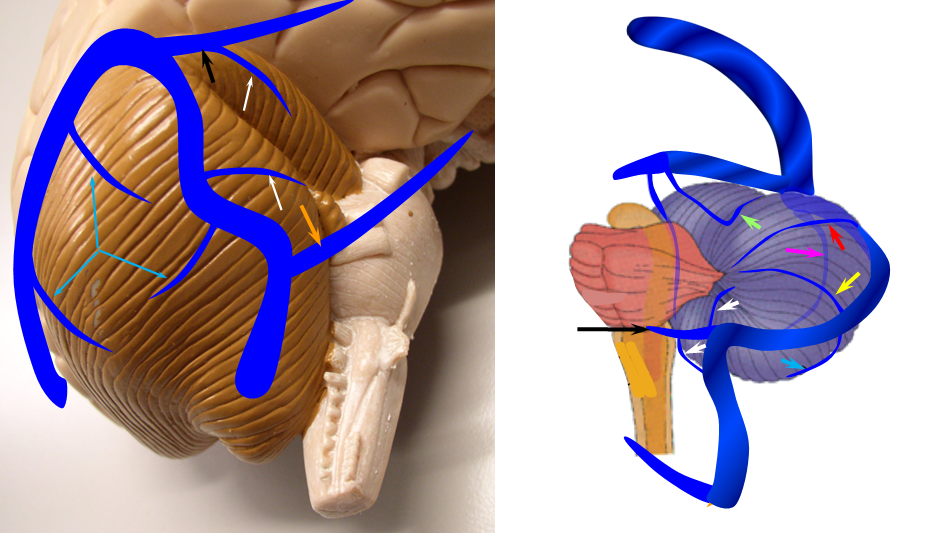
A diagram of cerebellar surface veins with respect to their sinus drainage. Understanding the relationships between the surfaces of the cerebellum and adjacent venous sinuses allows one to deduce the surface location of a cerebellar vein based on its point of drainage into the sinus system. A mesial superior surface vein (red arrow) will usually drain into the mesial portion of the proximal transverse sinus. A more lateral superior surface vein (yellow) tends to drain into the lateral aspect of the transverse sinus or proximal sigmoid. Anterior lobe veins (white) will typically open into the superior petrosal sinus (black), inferior petrosal sinus (orange), or sigmoid sinus. Inferior surface (blue) usually drains from the bottom into the transverse or sigmoid sinus.
Posterior inferior surface venous dominance
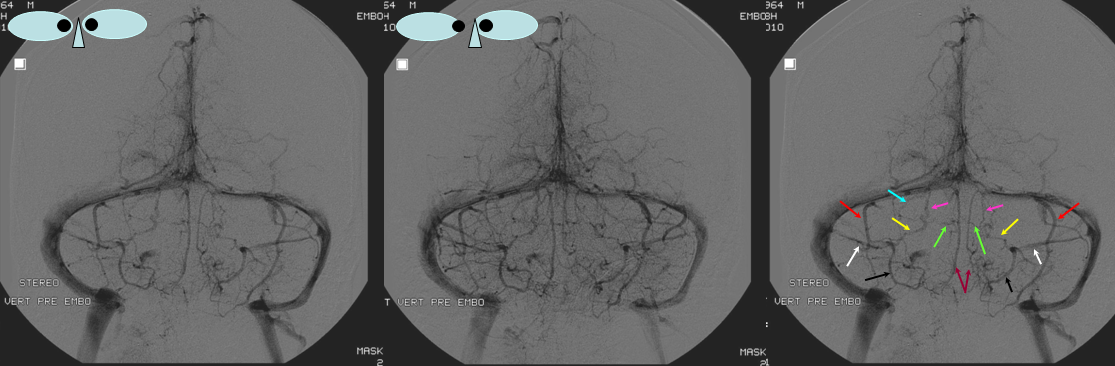
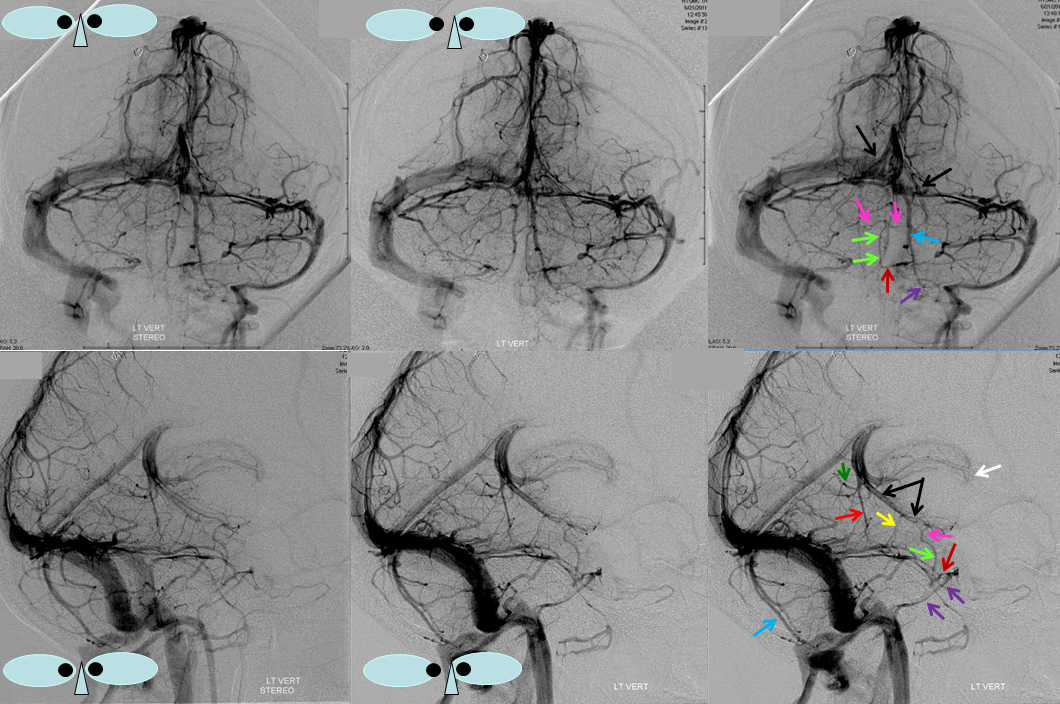
Symmetric appearance of dominant posterior inferior cerebellar veins (red), which must be posterior and inferior based on the location of their drainage into the transverse sinuses. Stereo images can be used for “confirmation.” Paired inferior vermian veins are labeled with brown arrows. Relatively smaller anterior surface cerebellar veins (black) drain into the mesial aspect of the superior petrosal sinus. Multiple other veins are visible. A left superior surface vein (unlabeled) is located next to the dominant inferior surface vein marked with red arrow. One disadvantage of the Townes view is that both superior and inferior surface veins project below the transverse sinus — in this case, the lateral projection becomes quite useful. Other veins are labeled as well — once the superior sagittal sinus (white) is recognized, the characteristic slanted projection of the petrosal veins (yellow), and their connection to the vertically oriented lateral mesencephalic veins (pink) is seen. The interpeduncular veins are labeled in green, relative to the basal veins (pink). The interpeduncular veins are hard to spot without the stereo.
Inferior Vermian and posteroinferior surface venous dominance
Dominance of inferior vermian veins (light blue), and to lesser extent posterior inferior cerebellar veins (dark blue), in drainage of the cerebellum. Small anterior surface vein is labeled in green. Superior petrosal sinus is red.
Another example of Inferior Vermian Vein Dominance — see how the veins are deep to the posterior hemispheric surface — as vermis is deep as well

Superior Vermian Dominance
Less common than inferior vermian for sure. But all part of a spectrum. In this person, superior vermian dominance is associated with corresponding hypoplasia of anterior (petrosal) and torcular groups
Video of T1 post volumetric MRI in same patient
Another dominant superior vermian vein angio and MR
Anterior surface venous dominance
Dominant anterior cerebellar hemispheric veins (red) emptying into the superior petrosal sinus, and superior vermian vein (dark blue) opening into the Galen. The superior vermian vein (dark blue) is prominent, as collector of the posterior superior surface drainage (balance, again). Inferior vermian vein is marked in orange. The lateral mesecephalic vein is white, and petrosal vein is purple. Basal vein is black. Superior petrosal sinus is light blue.
Superior cerebellar surface venous dominance
Vermis
Vermis is defined by superior and inferior vermian veins. Either can be dominant or co-dominant. The superior one usually drains either into the precentral vein (pink), in which case the proximal trunk (blue) is called the superior cerebellar vein. The inferior vermian vein (green, violet) usually drains into the torcular area. Well-defined cerebellar vermian veins like the one below outline the surface of the vermis, which is deeper than the hemisphere surface, and is the reason why the inferior vermian vein in particular spans the inner semi-circle relative to the more superficial inferior hemispheric veins (brown). The superior vein outlines the various relatively obscure names for different parts of the vermis, for example the declive (white, yellow), culmen (orange, red), separated by the primary cerebellar fissure with its corresponding vein (black)

Stereo:

Brainstem:
The brainstem veins are generally quite small in caliber, and exhibit high degree of variation. They are best visualized in the early venous phase — by the time the venous sinuses are well seen, the brainstem veins are becoming too washed out. So, better study them in the early venous phases, and connect with the sinuses either mentally or by superimposition.
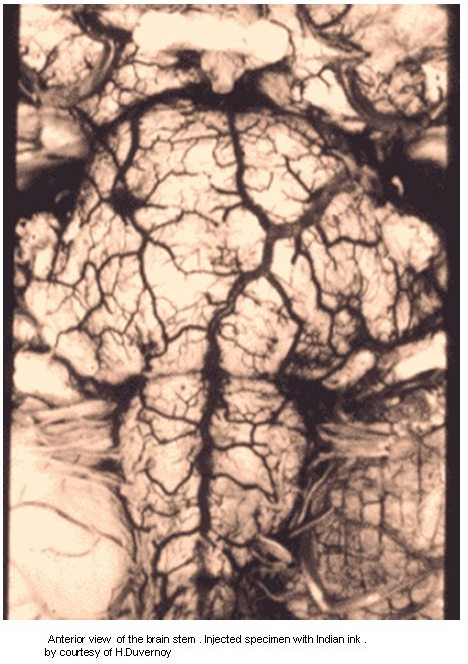
The above micrograph of an injected specimen shows a large network of small caliber veins surrounding the brainstem — with some consistently larger “named” channels. You can see how much busier and more distributed this network is, as compared with neat schematic drawings we have come to rely on. There is great variation, and dominance of one channel usually implies hypoplasia of its neighbors. For example, the lateral mesencephalic vein is pretty consistently identified on most injections, and the anterior mescencephalic vein is relatively smaller, except when the reverse is the case. One has to be careful, of course, not to confuse left and right on the lateral views, which can be difficult. Oblique views can help, but I find that it is more worthwhile to gain an understanding of these veins in the AP views — perhaps not as obvious at first, but ultimately very informative.
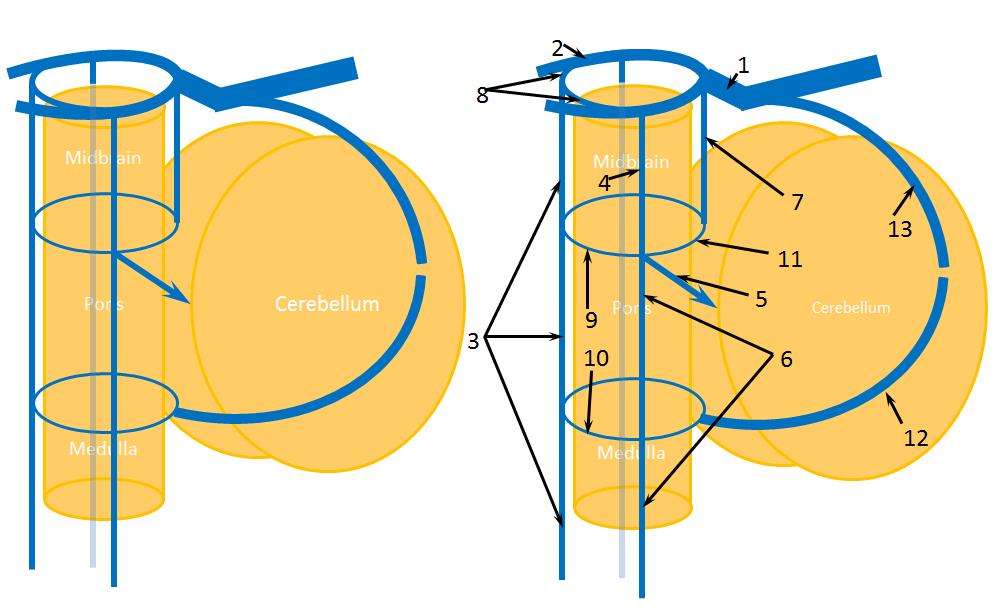
Figure X: Brainstem Veins. 1 – Galen; 2 – Basal Vein of Rosenthal (paired); 3 – anterior mesencephalic/pontomescephalic/pontomedullary/medullary vein conduit; 4 – lateral mesencephaic vein; 5 – petrosal vein, with arrow pointing to superior petrosal sinus; 6 – lateral pontine/lateral medullary vein conduit; 7 – precentral cerebellar vein; 8 – interpeduncular veins / posterior communicating vein; 9 – transverse pontine vein/pontomesencephalic sulcus vein; 10 – pontomedullary sulcus vein; 11 – brachial vein; 12 – inferior vermian vein (connects to pontomedullary sulcus veins via the tonsillar veins); 13 – superior vermian vein
You can conceptualize the brainstem as a cylinder (see above figure), with veins along its surface, like a kind of cage. At the anterior margin of the cylinder is the anterior pontomesencephalic/anterior medullary/anterior spinal vein line. It is the same channel, with different names depending on the adjacent brain structure and the source you are studying. Quite often, it is discontinuous. Lateral surface is dominated by the lateral mesencephalic vein which, contiguous with the petrosal vein, connects the basal vein to the superior petrosal sinus. The lateral mescencephalic vein is one of the most consistently present more important venous conduits. It is, theoretically, contiguous with the lateral pontine and lateral medullary veins, which are often quite small. Together, the lateral mesencephalic, lateral pontine, and lateral medullary veins constitute the lateral longitudinal venous channel of the brainstem. The back surface of the brainstem is a somewhat orphaned property. It is dominated by the precentral vein (a.k.a. precentral cerebellar vein, a.k.a. pre-central vein, etc.). Although it receives most of its venous content from the cerebellum (running along the anterior superior vermian surface), it may be connected with the lateral mesencephalic/pontine/medullary channel via a series of transverse veins which are desribed below, and thus participates to some extent in drainage of the brainstem.
The above-mentioned three dominant longitudinal venous channels are connected by a series of transverse veins, which run in more or less axial plane. At the top, the interpeduncular vein connects both lateral mesencephalic veins. In the middle, the pontomesencephaic / transverse pontine vein (sometimes depicted in the pontomescencephalic sulcus, and sometimes in the midpons, and realistically present in both places depending on the specimen) may connect the anterior mesencephaic, lateral mesencephalic, and precentral veins. Inferiorly, the pontomedullary sulcus vein may be a more prominent venous channel running in the sulcus of its name. Having said all that, in practice you will find several of these veins to be relatively dominant while the rest are small enough to be angiographically invisible. Again, it cannot be overemphasied that the venous network is a highly variable lattice of conduits, some of which, by virtue of relative prominence, have been named and thus canonized, with detrimental consequences to the more realistically appropriate emphasis on variation. This is where understanding relationships between veins, sinuses, and arteries can help you in identifying how these channels are located relative to adjacent brain structures. This kind of understanding is best achieved by persistent staring at many venograms, with no effective substitute for this approach.
Here is an example
Lateral Mesencephalic Vein / Petrosal Vein
Lateral mesencephalic vein (blue) draining an AVM supplied via anterior inferior and superior cerebellar arteries. It is almost always identifiable on noninvasive routine imaging. IAC studies are good for brainstem veins (CISS and such sequences).
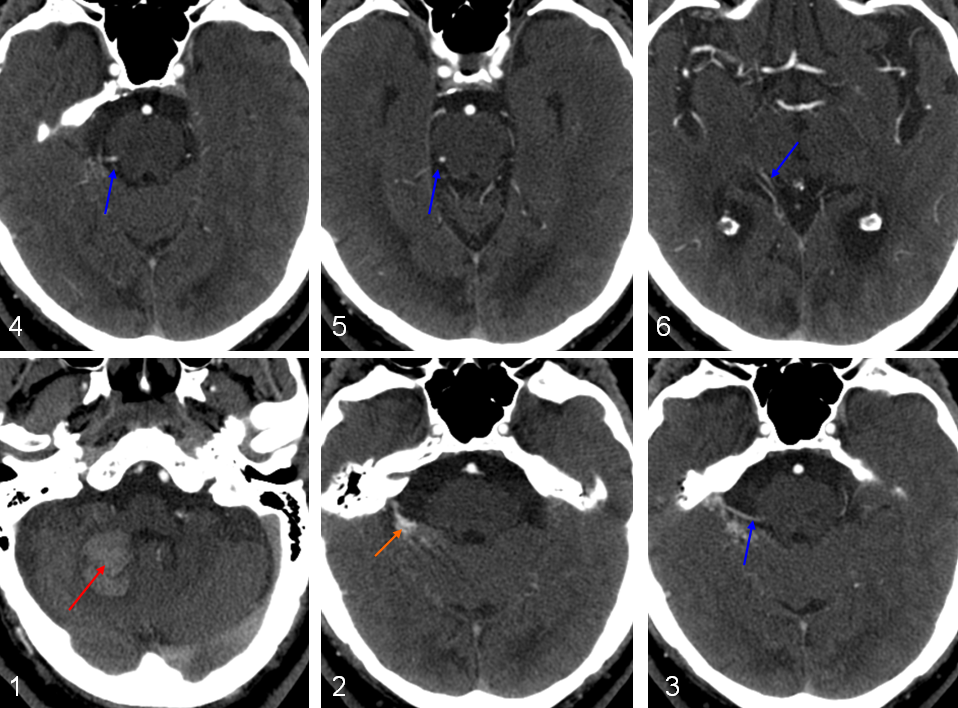
CT: 1-6 showing a hematoma (red) associted with an anteromedial surface avm (orange) drained via the lateral mesencephalic vein into the basal vein of Rosenthal.
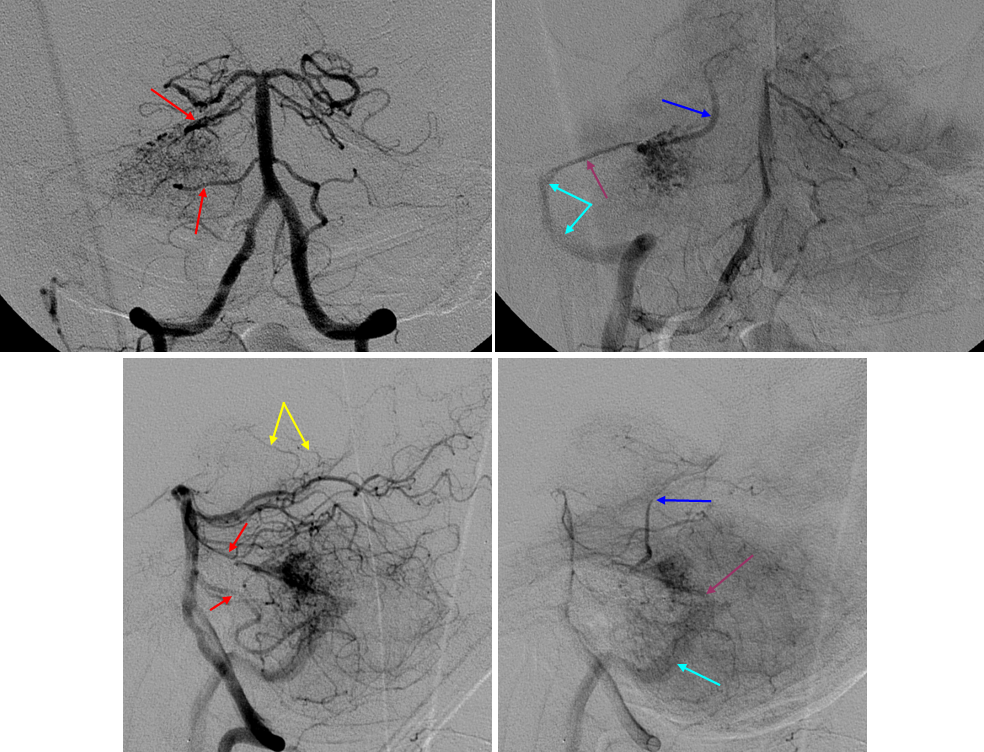
Angio of the same case showing AICA and SCA (red) supply to the avm, with “deep” drainage via the lateral mesencephalic vein (blue) emptying into the basal vein, as well as cortical cerebellar surface vein (purple) emptying into the sigmoid sinus (light blue). Notice bilateral AICA-PICA disposition and typical appearance of the posterior medial choroidal arteries (yellow)
Petrosal Vein
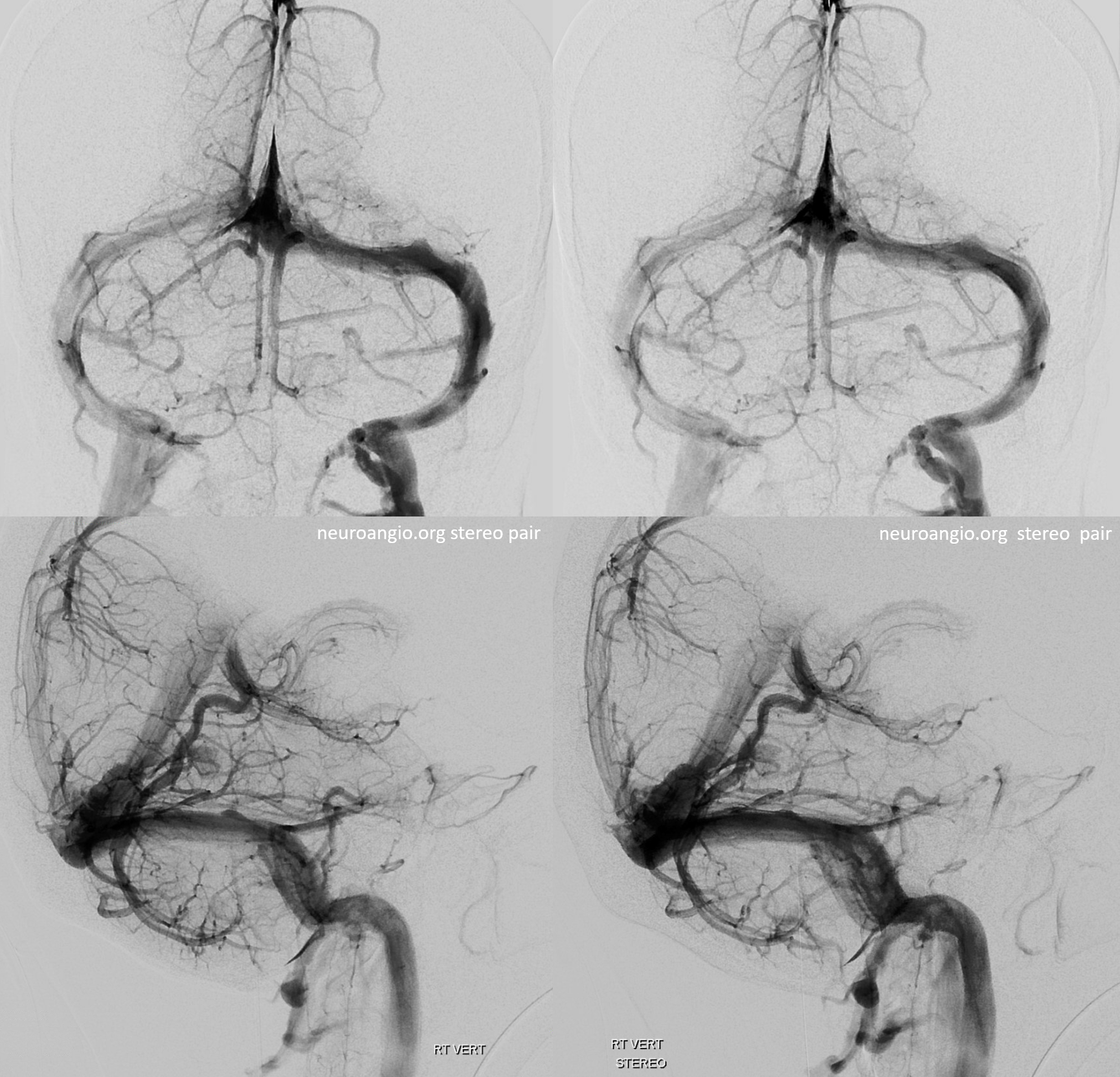
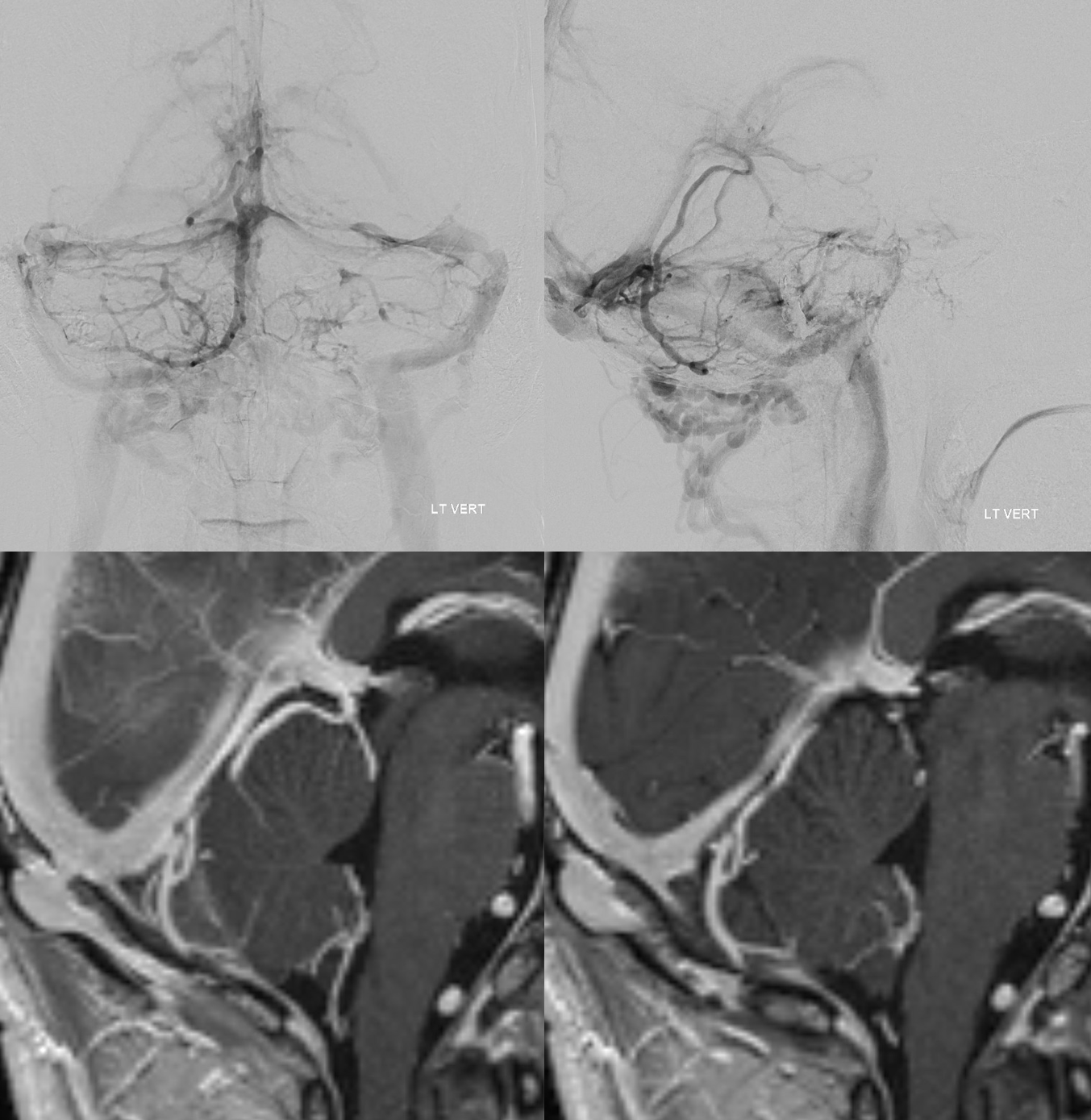
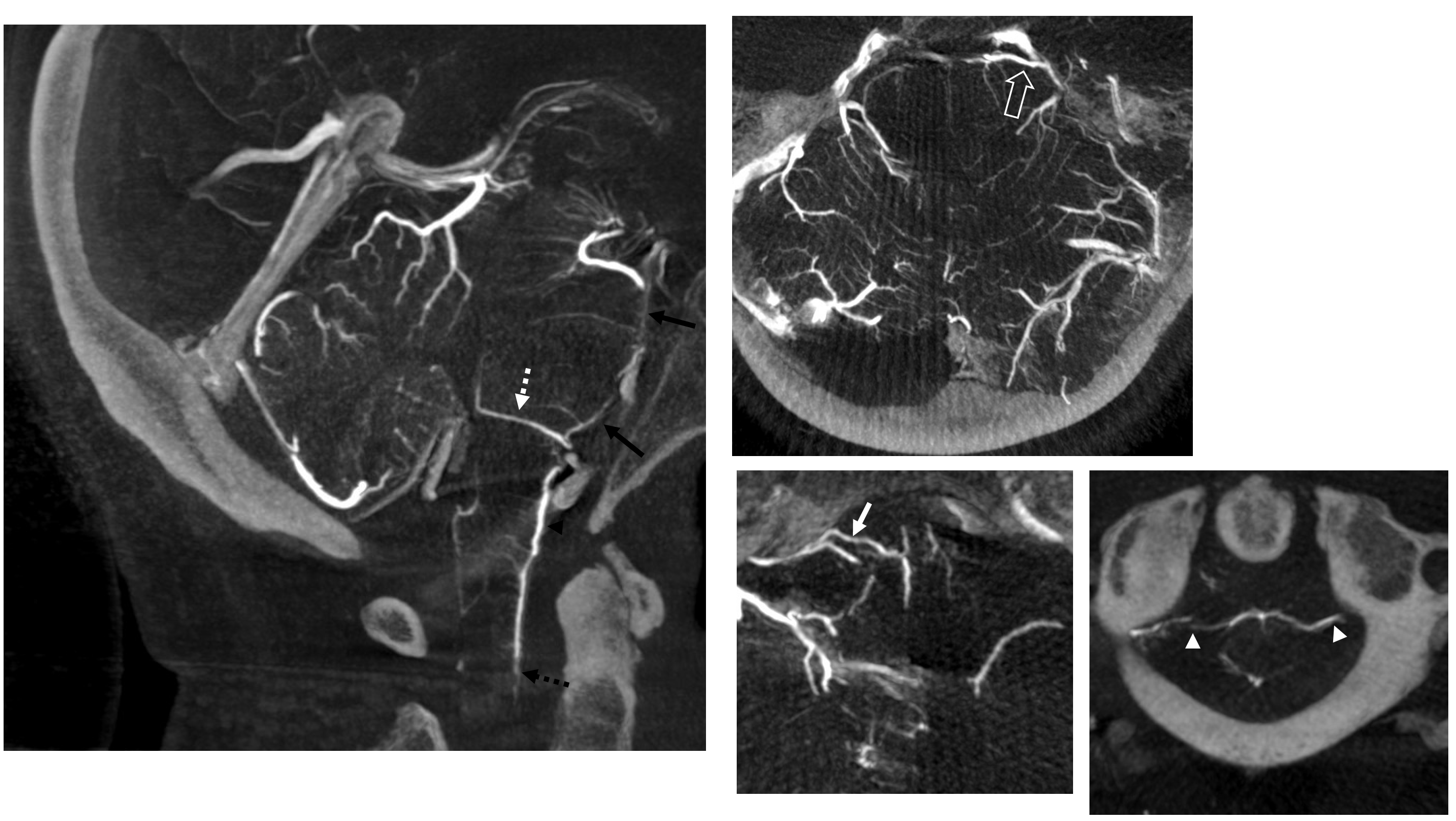
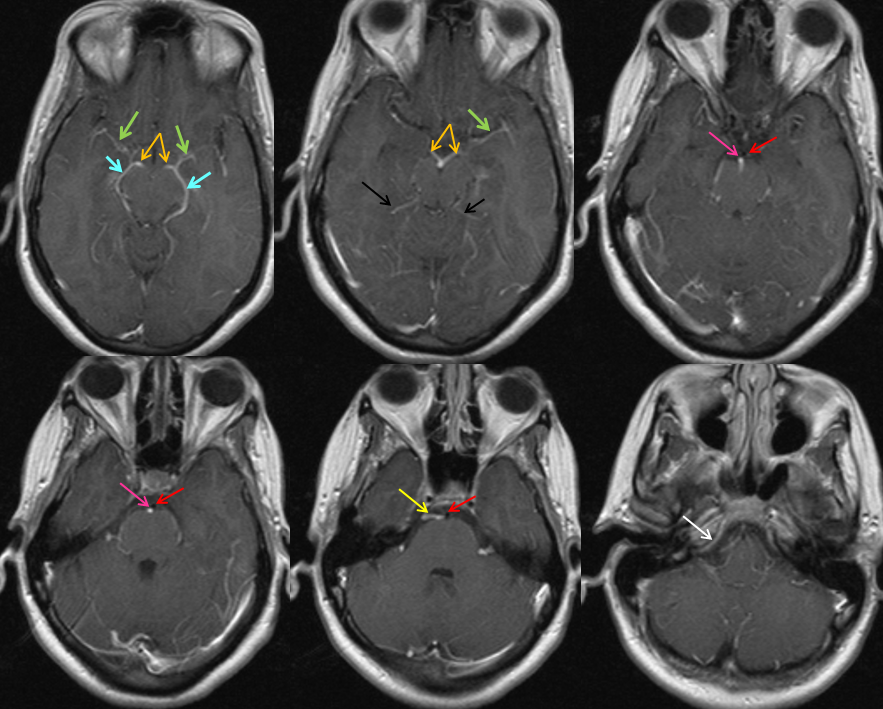
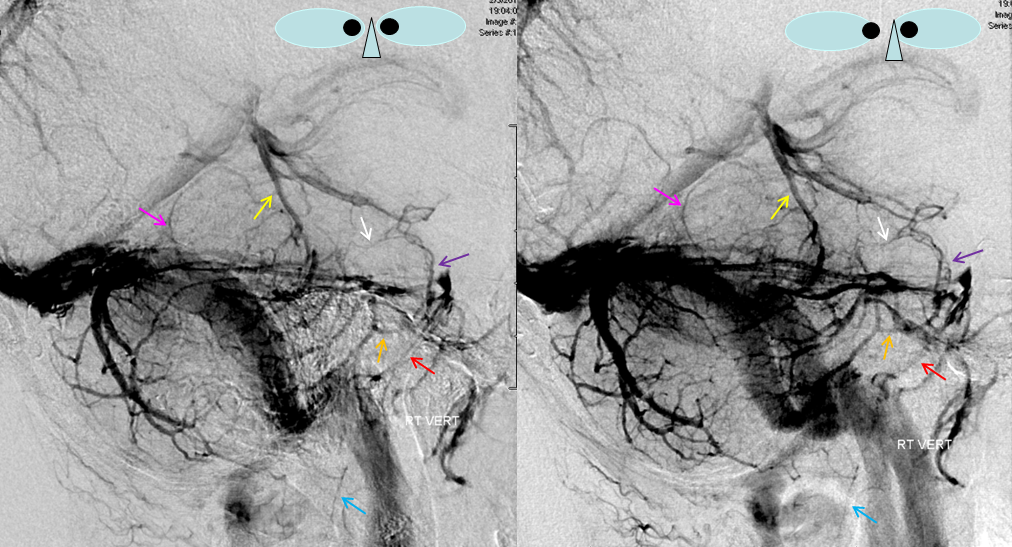
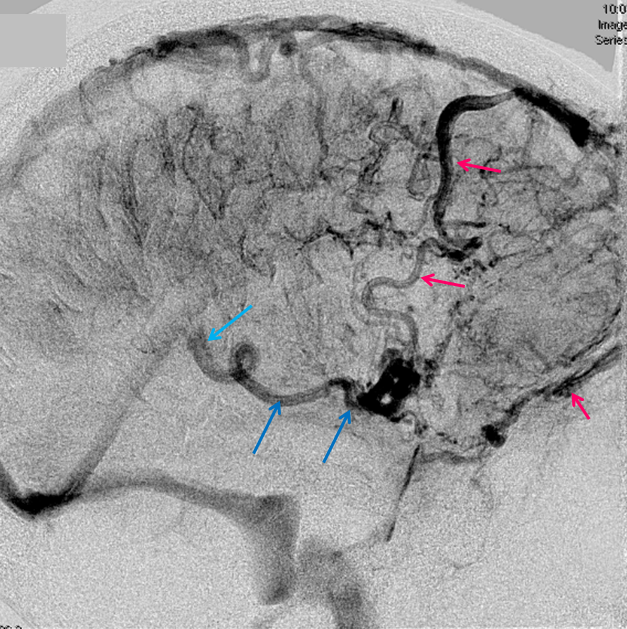
This key vein is strategically situated to collect tributaries from the anterior and lateral brainstem surfaces, and from anterior superior and inferior cerebellar surfaces. As such, it is almost always visible angiographically and on cross-sectional imaging, more or less prominent to the extent that it captures the aforementioned territories. As with all posterior fossa veins, I think that a motivated learner is best served by first identifying these veins on cross-sectional imaging (contaminated CTA, CTV, contrast CT, or MRI postcontrast T1 sequence). Whatever input the petrosal vein receives, it will usually drain into the superior petrosal sinus. This structure, in itself, is a conduit between the cavernous and sigmoid sinuses, just like the basal vein is a conduit between the cavernous sinus and the vein of Galen. And, just like in the case of basal vein, the superior petrosal sinus can be partially hypoplastic, such that the petrosal vein may drain posteriorly into the sigmoid sinus (more typical), or anteriorly into the cavernous sinus (less typical). This is illustrated in the example below, where the petrosal vein (green, pink arrows) drains via the posterior aspect of the superior petrosal sinus (dark blue arrows) into the sigmoid sinus on the left, and cavernous sinus (yellow) via the anterior portion of the superior petrosal sinus (black arrows) on the right. Also seen are superior (white) and anterior inferior (light blue) cerebellar venous tributaries to the petrosal vein on the left, and the lateral mesencephalic vein (red) on the right. The posterior portion of the cavernous sinus empties into the inferior petrosal sinus on the right (purple arrows) It is a beautiful set of images when seen stereoscopically, and rather crowded especially for students without that capability.
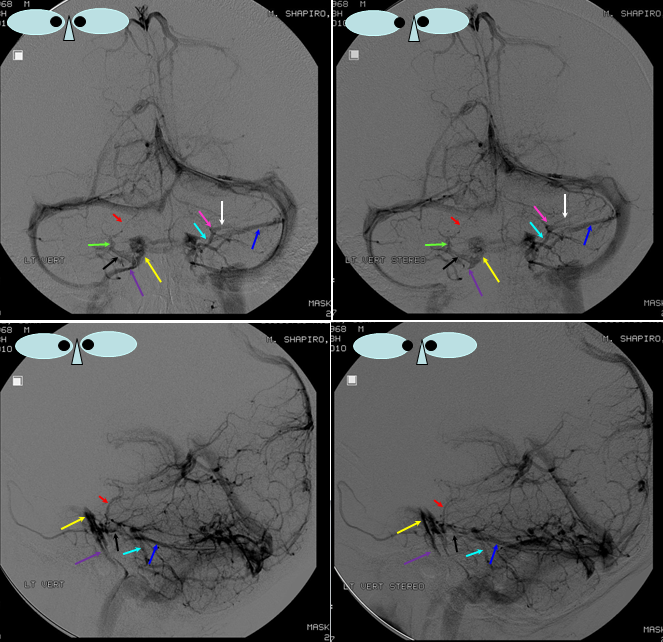
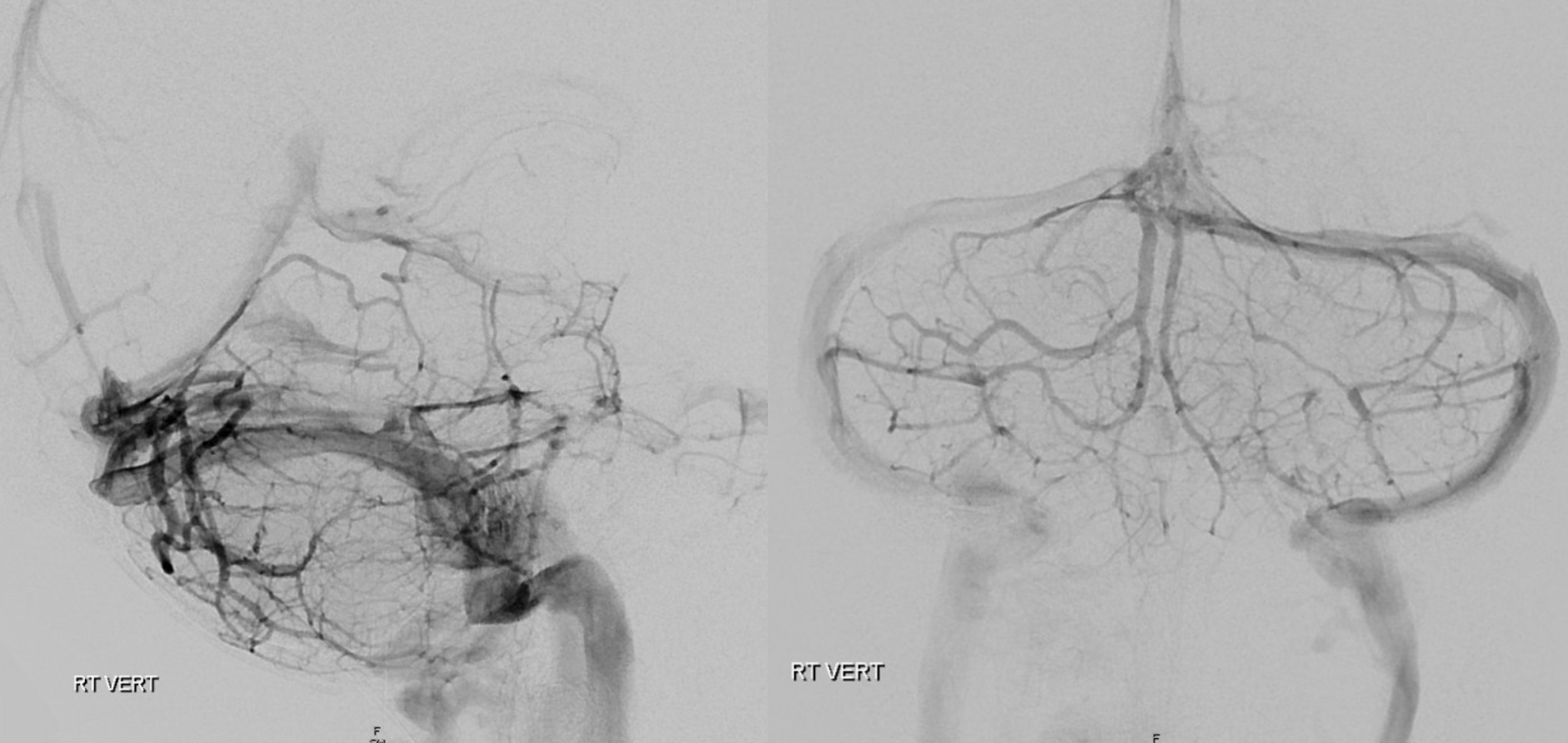
The same images are shown without the arrows, for further viewing clarity.
Transverse Pontine and Lateral Mesencephalic Veins
Lateral mesencephalic vein (red); Basal vein (black, hypoplastic on the right, which is the side of the large lateral mesencephalic); interpeduncular vein (yellow), which is typically located at the anterior margin of the basal vein (black) component visualized on posterior fossa injections; anterior pontomesencephalic vein (blue); transverse pontine vein (dark green) will be located somewhere at the level of the superior petrosal sinus, and runs parallel to the basal vein. Thus, the basal, lateral mesencephalic, anterior pontomesencephalic, and transverse pontine veins outline the brainstem (red, yellow, blue, green arrows). White — precentral vein. Purple — inferior vermian veins.
Anterior Mesencephalic Vein — this vein runs in front of the mesencephalon. It forms part of the ventral venous axis which runs from anterior spinal to premedullary to anterior pontomesencephalic veins (see above diagram). Usually, the lateral mesencephalic is the dominant conduit of midbrain drainage. In this patient, the anterior mesencephalic vein (light blue arrows) is particularly well-developed, draining into the basal vein (dark blue arrows). The entire ventral axis, though — pontomesencephalic (light blue) to premedullary (white) to anterior spinal veins (black)– is visible. The very early arterial phase image is chosen for the “mask”, allowing the anterior pontomesencephaic vein to project next the to basilar artery, which is seen in white. The lateral mesecephalic vein (yellow) is also well seen in its vertical orientation, as compared with the more obliquely, laterally oriented petrosal vein (brown) which, in this case, also receives the transverse pontine vein (red). As usual, it is much easier to appreciate these veins in stereo, particularly given superimposition with cerebellar veins. A good example of the precentral vein (pink) is also seen.
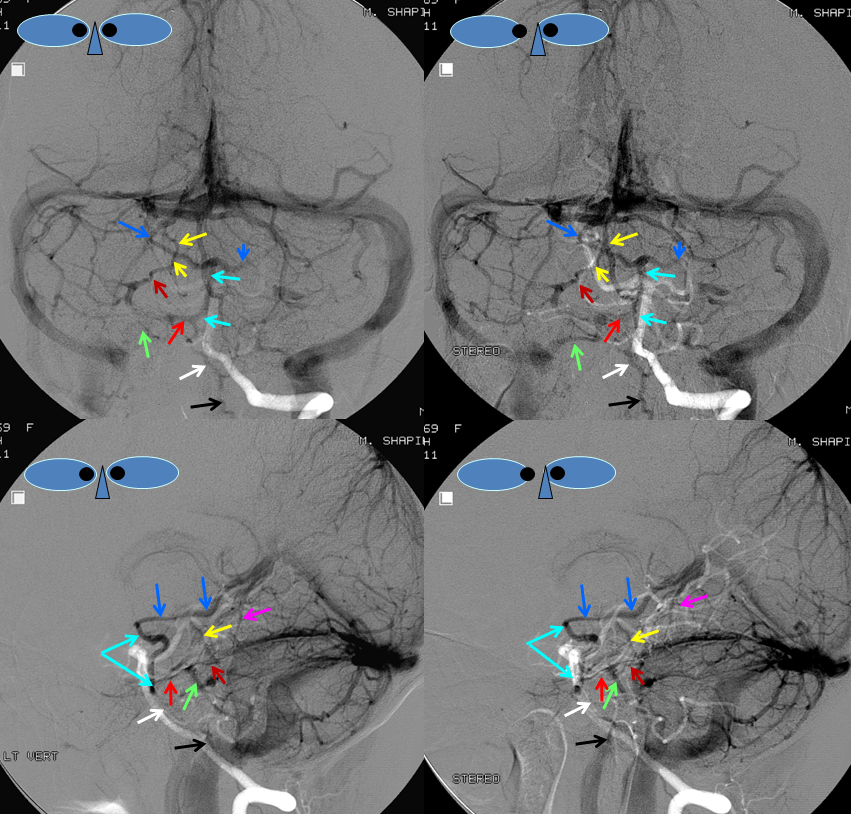
Same image with no labels, for ease of visualization.
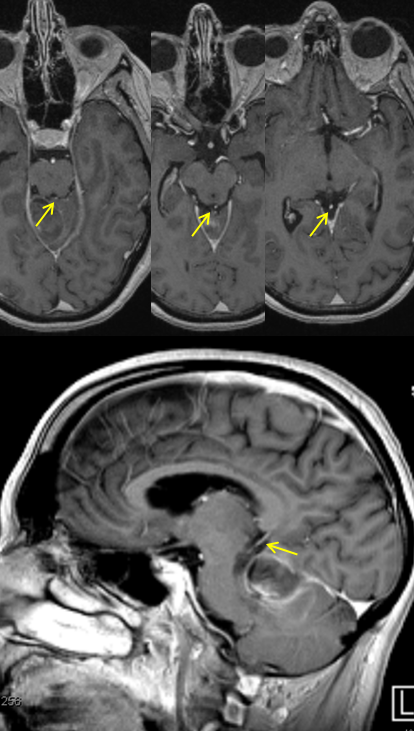
MRI of the same patient, demonstrating the anterior pontomesencephalic vein and other regional veins. Again, the veins are often best seen on a plain post-contrast T1 sequence, especially when its volumetric. TOF venous studies have some advantages, and many more drawbacks. Basal vein – light blue; Interpeduncular (posterior communicating) veins – orange; anterior pontomesencephalic vein – pink, next to the basilar artery (red); the pontomescephalic vein drains into the petrosal vein (yellow) and then into the inferior petrosal sinus (white). The deep sylvian (middle cerebral) veins are green, and atrial veins are black.
Brainstem veins in patient with CP Angle mass
A large left CP angle schwannoma has compressed the neighboring veins, resulting in some instructive re-arrangements. How did the patient present? Answer at end of this case. Lateral pontomesencephalic vein is shown with yellow arrow.

Venous phase of right vertebral artery injection. The petrosal group is absent on the left. Cerebellum drains via posterior and superior surface veins. Pons and medulla drainage is collected into a large anterior pontine vein (bright blue), contiguous with anterior medullary / anterior spinal vein (violet) which drains into a C1 foraminal vein (orange). Notice also nice demonstration of the interpeduncular vein right and left aspects (pink) with the posterior-most portion located in the interpeduncular fossa (white). On the left, the interpeduncular vein drains into a posteriorly-directed basal vein (yellow), whereas on the right the basal vein (black) drains anteriorly towards the cavernous sinus.

Detail of interpeduncular vein anatomy, same arrows as above.

The patient presented with visual complaints due to papilledema. Crystal clear elevation of the optic nerve heads is seen on this CISS sequence (pink arrows). Fluid is seen in the optic nerve sheath complex (yellow) however this is highly nonspecific. The temporal horns are “up”. This is obstructive hydrocephalus due to compression of the aqueduct of Sylvius, as is also seen in this image.

Anterior group of brainstem draining veins
The anterior axis of the anterior mesencephalic/pontine/medullary/cervical veins goes by various names such as anterior pontomesencephalic, anterior pontomedullary, etc. The important point is to understand how the brainstem is draining. Again, similar to the disposition in the supratentorial compartment, relative prominence of one venous group such as Labbe implies proportional hypoplasia of the others (such as Trolard). The same is true of the brainstem, except that the veins are smaller, networks more distributed, and tolerance for occlusion is greater. Hence the surgical teaching in some institutions that one can always “take” the petrosal vein. That is almost always true because of the greater inter-connectedness of brainstem veins — certainly much more so than with the lateral convexity veins. But not always. Which is why it does not hurt to have that presurgical angiogram….
Here is an example of a patient with a very prominent anterior medullary (bright blue) / anterior cervical (dark blue) venous conduit. The prominence of cervical veins is due to hypoplasia of the normal drainage of the anterior system into the petrosal vein. Instead, the medullary vein decompresses into the anterior cervical vein, and subsequently via multiple bridging veins (green) into the neural foraminal venous plexi (purple), as is typical of spinal veins. Also well seen is the usually quite hypoplastic posterolateral or posterior spinal vein (yellow). The veins of the cord are much more interconnected than spinal cord arteries, even at the level of the cervical ford where a well-developed lateral spinal artery is common. Also please note a well-seen inferior vermian vein (purple), formed by its main tributaries the superior and inferior tonsillar veins (brown) which outline the posterior aspect of the cerebellar tonsil.

The same case, in native views. Notice on the lateral view how close the posterior aspect of cord is to the back of the relatively hypolastic atlas bone in this patient (look at the thin sliver of the posterior spinal vein, no labels here). Keep that in mind next time you are asked to do a C1 puncture.

Precentral (Cerebellar) vein. An unpaired vein running in the cistern of the same name, behind the brainstem, to empty into the superior vermian vein or the Galen. An important angiographic landmark, identifying the back of the brainstem. Prior to development of cross-sectional imaging, it served as a crucial weathervein for various posterior fossa mass effects — being unpaired and located between the brainstem and the cerebellum made it pretty much ideal for judging what was pushed from where. Still just as useful, but being quickly forgotten.
A relatively prominent precentral vein (yellow), as seen on CT and angiogram of the same patient. Notice, please, that promience of the precentral vein is associated with hypoplasia of the lateral mesencephalic veins, as explained above. The anterior pontomesencephalic vein (purple) is also more promienent than usual, again reflecting a balance with the lateral mesencephalic conduit. Other veins of note — the interpeduncular vein connecting both basal veins [unlabeled, for once :-), above the purple arrow, connecting the basal veins and better seen in the image on the right], transverse pontine vein (orange), hypoplastic superior vermian vein (pink), and inferior petrosal sinus (red). The anterior spinal vein is marked in light blue.
The inferior aspect of the precentral vein defines the upper border of the 4th ventricle, which is another key anatomical landmark to keep in mind. This is best seen on MRI.
Brainstem Veins, balanced view. Notice how very wispy these veins are. It takes some training and pattern recognition to learn to see them.
A nice view of upper brainstem veins, again in stereo, to correlate with the diagram below (if you cant see stereo, look on the image ot the right, where anatomy is more clear). The anterior mesencephalic vein (black, 3) is caudally connected with the transvese pontine vein (beige, 9), and rostrally to the interpeduncular (a.k.a. posterior communicating) vein (dark blue 8, connects both interal cerebral veins, which are labeled in white 2). Lateral mesencephalic vein is red (4). Superior petrosal sinus is yellow, inferior is orange, inferolateral cerebellar vein and inferior vermian vein are green (12), superior vermian vein is brown (13), and precentral vein is pink (7).
Figure X: Brainstem Veins. 1 – Galen; 2 – Basal Vein of Rosenthal (paired); 3 – anterior mesencephalic/pontomescephalic/pontomedullary/medullary vein conduit; 4 – lateral mesencephaic vein; 5 – petrosal vein, with arrow pointing to superior petrosal sinus; 6 – lateral pontine/lateral medullary vein conduit; 7 – precentral cerebellar vein; 8 – interpeduncular veins / posterior communicating vein; 9 – transverse pontine vein/pontomesencephalic sulcus vein; 10 – pontomedullary sulcus vein; 11 – brachial vein; 12 – inferior vermian vein (connects to pontomedullary sulcus veins via the tonsillar veins); 13 – superior vermian vein
Tentorial Leaf Dural Sinus
These anatomical variants are more frequently encountered in the supratentorial brain (maybe simply because there is more brain tissue there). Not infrequently a domiant vein of Labbe will drain into a dural sinus before joining the sigmoid. This disposition is a curiosity with little clinical significance except in some surgical instances where removal of the dura may result in inadvertent venous compromise. In this case, the dural channel (pink) is located on the undersurface of the tentorial leaf (because it is draining the cerebellum). It collects tributaries (blue) from the superior ceerbellar surface and joins the proximal left transverse sinus, as best seen on the right lower lateral oblique image.

Applications:
Sturge-Weber Syndrome, a.k.a. Encephalotrigeminal Angiomatosis
SWS is part of a family of neurocutaneous disorders, characterized by abnormalities of ecto- and endoderm. The cutaneous part is a port wine stain (in CN V distribution). The brain part is described below. About 1/3 of patients only have the skin part, 1/3 have only brain, and 1/3 both — no rocket science here. The cause is unknown. There are many sources of excellent information on the Web, but I am afraid that most individuals do not appreciate the underlying vascular issues of SWS in the brain, which is illustrated angiographically below.
Cerebral manifestations of SWS appear to stem from abnormal development of the venous system — particularly surface veins. The halmark of venous imaging is absence of superficial veins (including basal vein, which is only deep as far as the surgeon is concerned, being in fact a superficial vein on the undersurface). As a result, venous drainage is impaired, with secondary tremendous venous congestion. The congestion leads to engorgement of countless small veins thoroughout the parenchyma, and particularly on the gyral surface. This produces the characteristic gyral enhancement seen on MRI, and venous congestion that is better appreciated angiographically. The characteristic gyral calcifications probably result from chronic venous congestion.
This is a young patient with intractable seizures.

x-ray views of the skull, showing extensive gyral calcifications on background of cererbral atrophy.
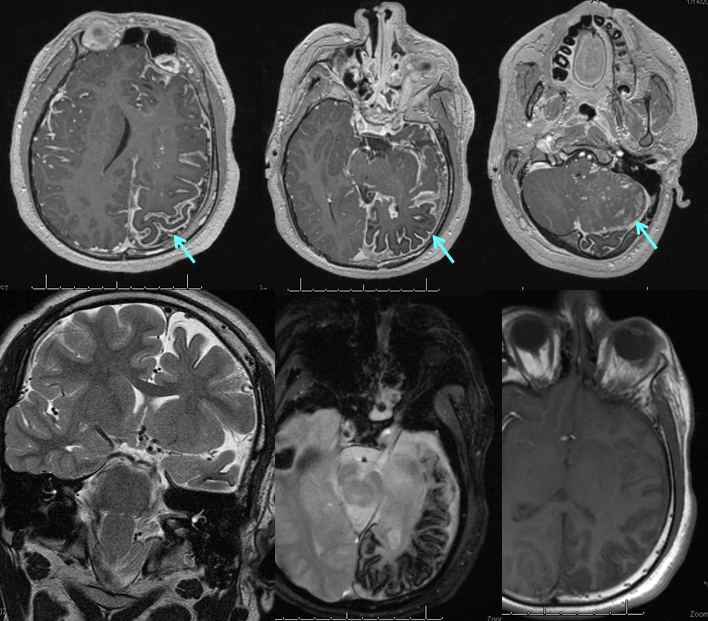
Various MRI sequences highlighting atrophy, calcifications, and gyral pattern of enhancement (top row). Notice absence of left basal vein, and most surface convexity veins.
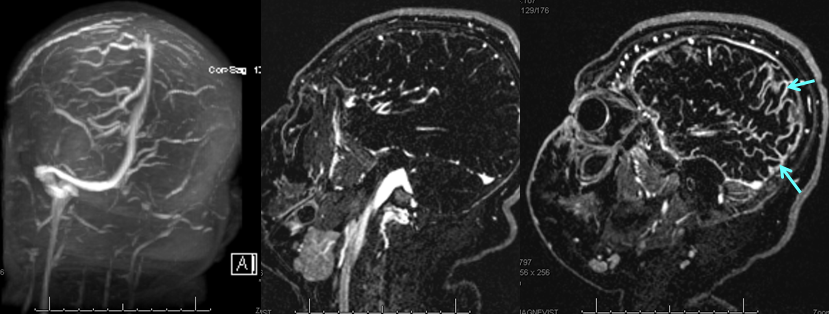
TOF and venovibe images; almost normal venous pattern on the right, and gyral enhancement (arrows) as well as transosseous venous channels on the left.
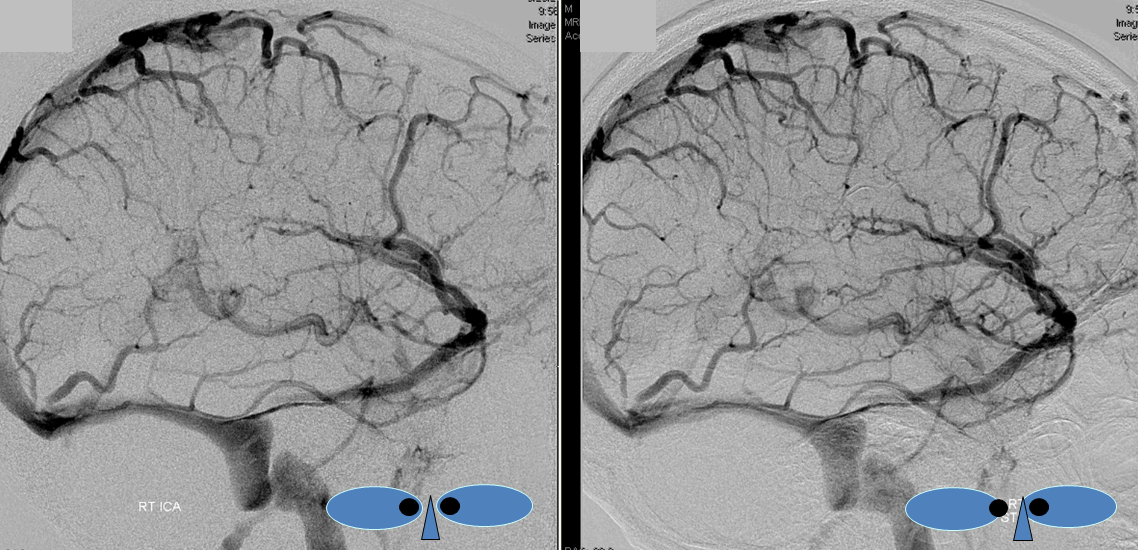
Stereoscopic views (top) and labeled image (bottom) of quasi-normal right ICA injection; convexity surface veins are present. A tremendous, tortuous basal vein (blue arrows) is working overtime. Some of its lenticulostirate tributaries, pathologically enlarged (why?) are labeled yellow. The convexity drainage is dominated by superficial sylvian veins (purple). What vein is missing?

The same R ICA injection, in AP projection. Notice multiple venous channels draining the anterior frontal lobe over the left convexity. They are intra-osseous veins, and well seen on the venovibe MRI image of the left hemisphere (no labels on that one). The basal vein is blue, and its deep tributaries are yellow. The internal cerebral vein is missing. Its territory is drained by the basal vein. I don’t understand the developmental physiology of why it is missing.
This is a lateral view of the abnormal hemishere, left ICA injection, in late venous phase. The image is characterized by near-complete absence of surface veins and tremendous venous congestion. Appreciate how gyral calcifications, seen on the x-ray image above, are greatest over the areas with least superficial venous drainage. Over the frontal lobe, where several surface veins (pink) have developed, the calcifications are less pronounced. The basal vein is labeled in blue. Why is the basal vein seen?
AP views of left ICA injection. The basal vein seen on the lateral study belongs on the right side. It is draining both hemispheres, hense its large size. Left-sided tributaries (green arrows) reach the right side accross the posterior communcating vein (interpeduncular vein) which connects the two basal veins in front of the brainstem.
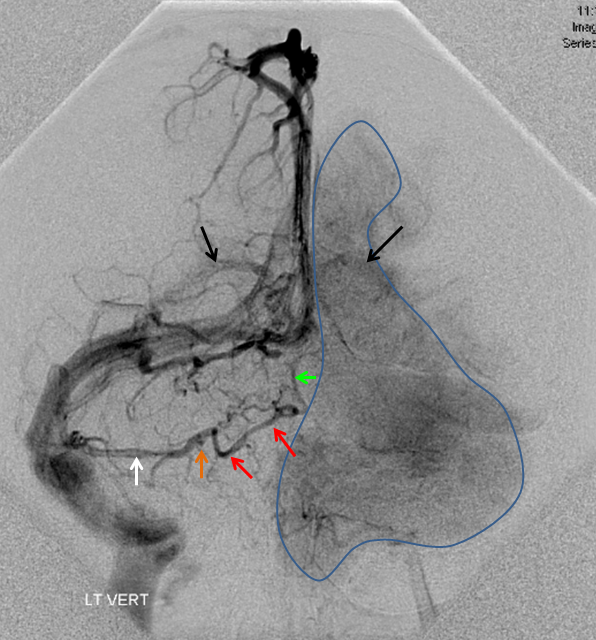
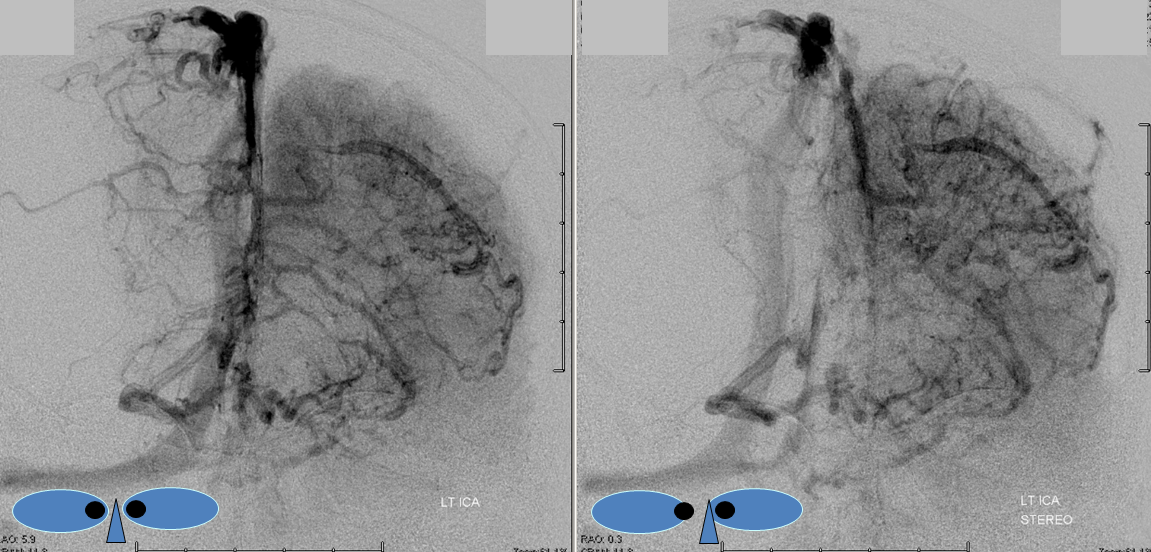
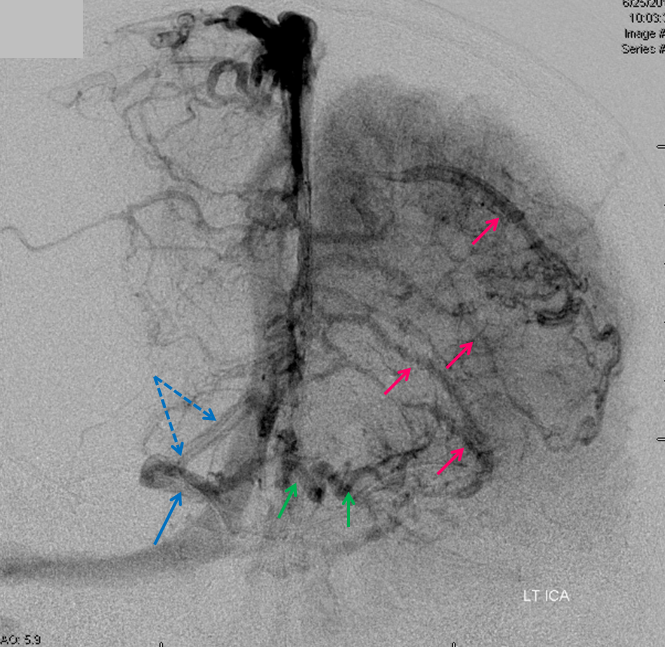
The disease is not limited to anterior circulation. Even more tremendous venous congestion (blue outline), wtih no effective surface veins, afflicts the left cerebellum, brainstem, and posterior cerebral artery territory, in stark contrast with normal right side. The brainstem drains almost exclusively via a large lateral mesencephalic vein (red), into the petrosal vein (beige), and ultimately into the superior petrosal sinus (white). An anterior mesencephalic vein (green) points straight up from medial aspect of lateral mesencephalic vein.
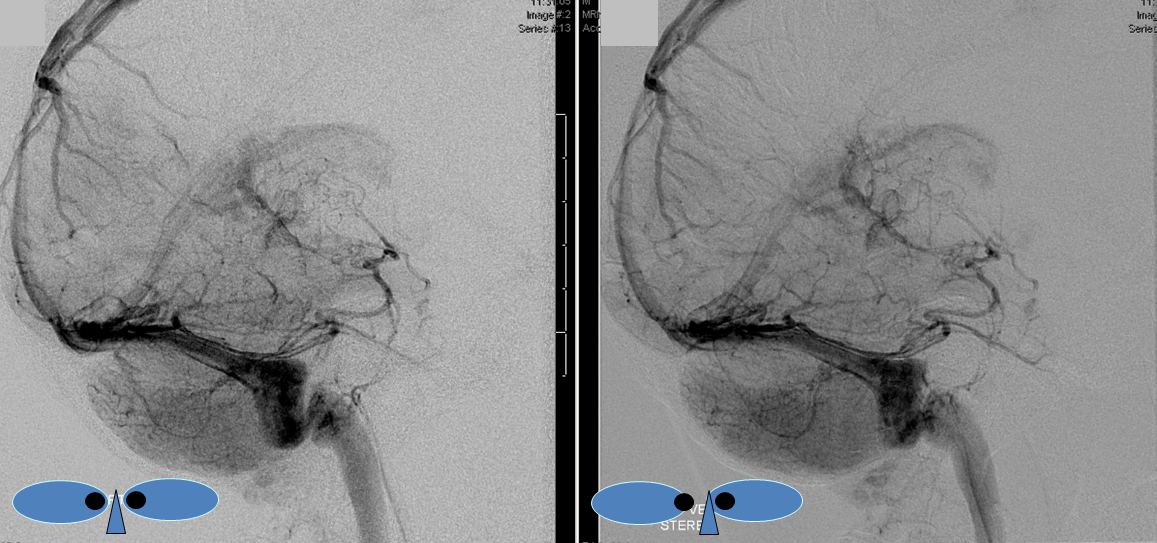

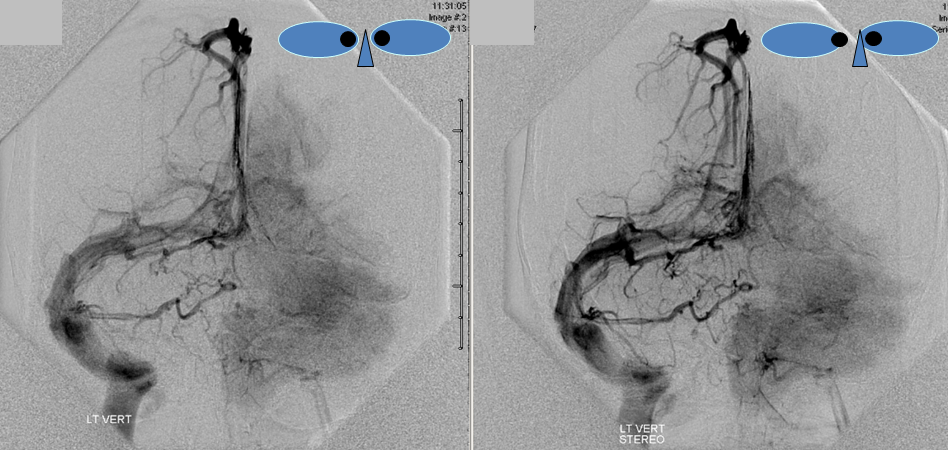
Lateral view of the same left vert injection.
Movies of vert injection are shown below