
Neuroangio.org does bony spine! Welcome to the Best Spine Center in the Galaxy! Here, we take on the toughest, most complex cases in the Milky Way. When YOUR fusion fails, call us at 212-263-6008 anytime. Operators are standing by!
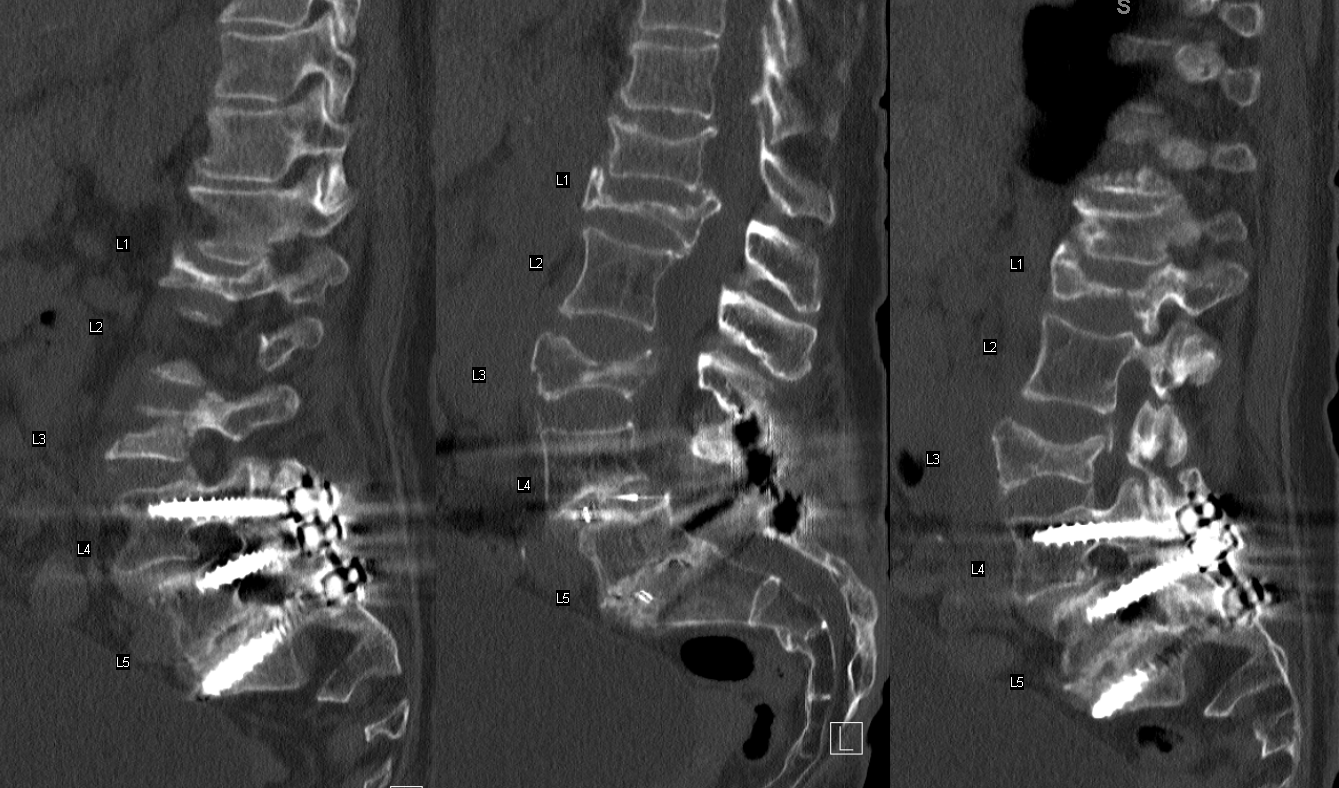
Seriously, though, we also do spine. And pretty complex spine, too. Not all kypho is hum-drum work, you know. Check out this patient with advanced spinal disease, prior lower lumbosacral fusion, with co-existing osteoporosis and subsequent several compression fractures, and severe progressive pain
Yet another fracture at T9, treated with kypho

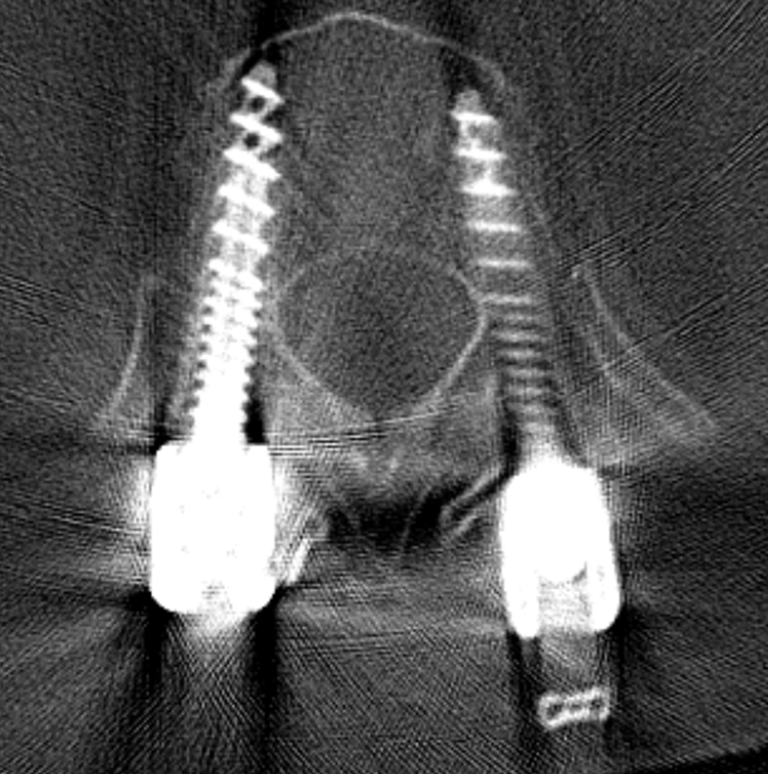
The fusion is extended to T11. Notice relative lack of cement around the right fenestrated screw
Same on axial
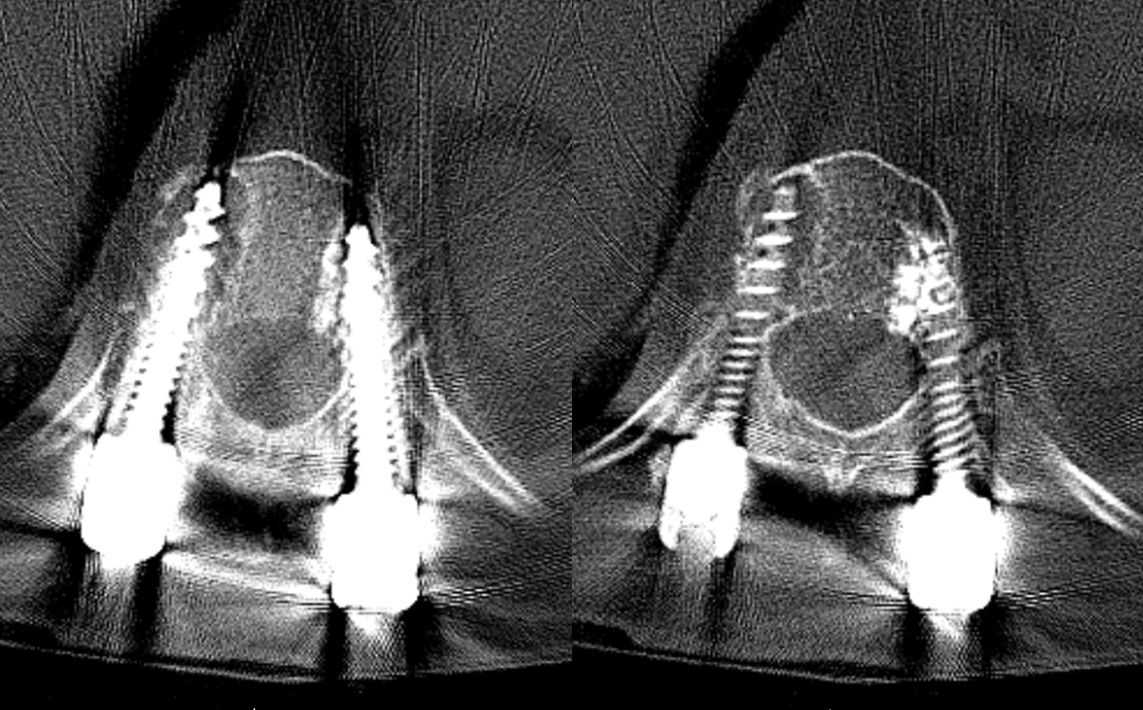
A few months later, thoracic pain is suddenly worse. There is a new T10 fracture and halo around T11 screw

Axials
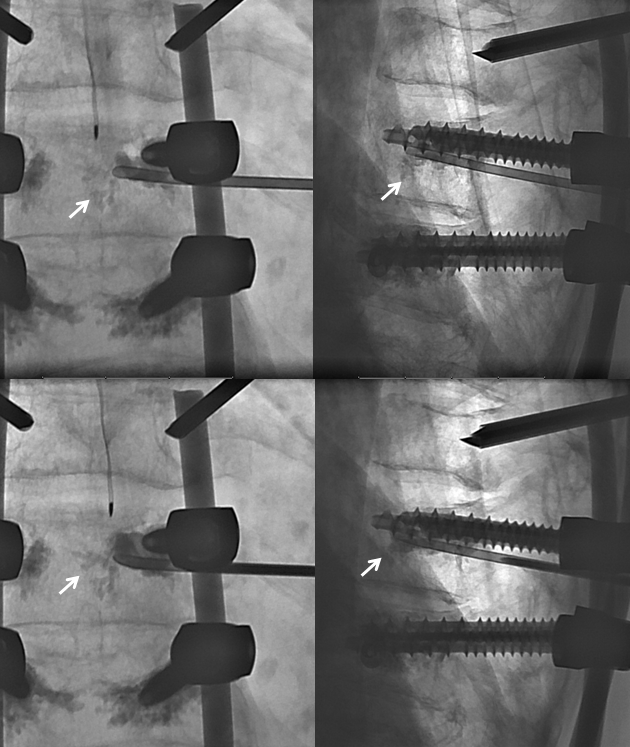
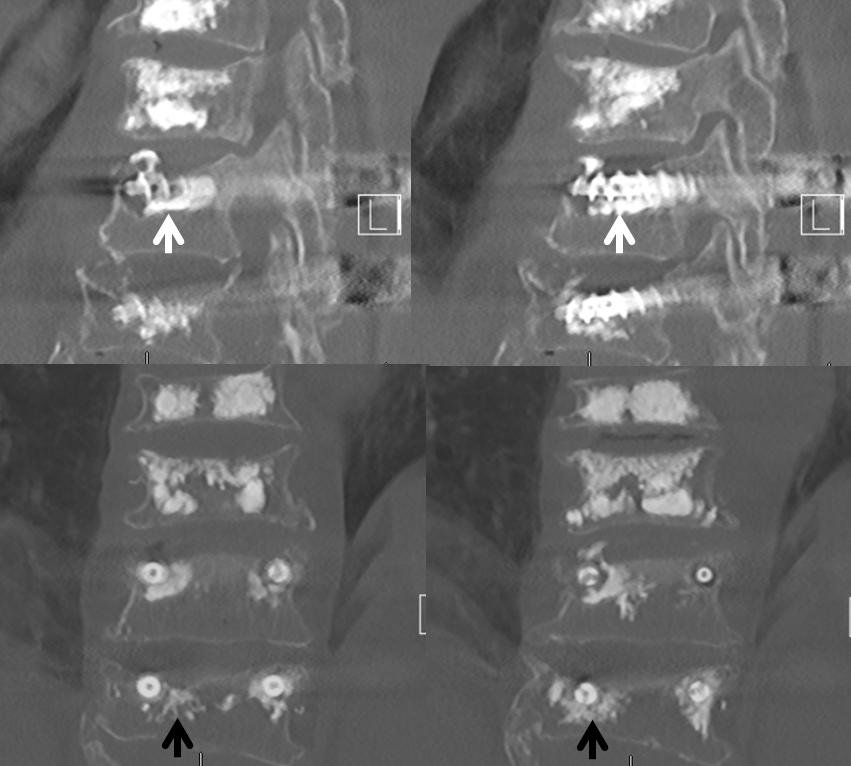
Decision is to try percutaneous augmentation and fill the void. An oblique frontal view (image on right) is chosen to slide a 22 gauge general purpose needle (white arrows) from lateral to medial under the screw. The bottom of the pedicle is shown by black arrow. Once the needle is in desired position, the frontal oblique is aligned exactly with the needle. Now all we have to do is put a bigger needle down the same trajectory. No need for CT, fancy guidance, etc. Just plain fluoroscopy
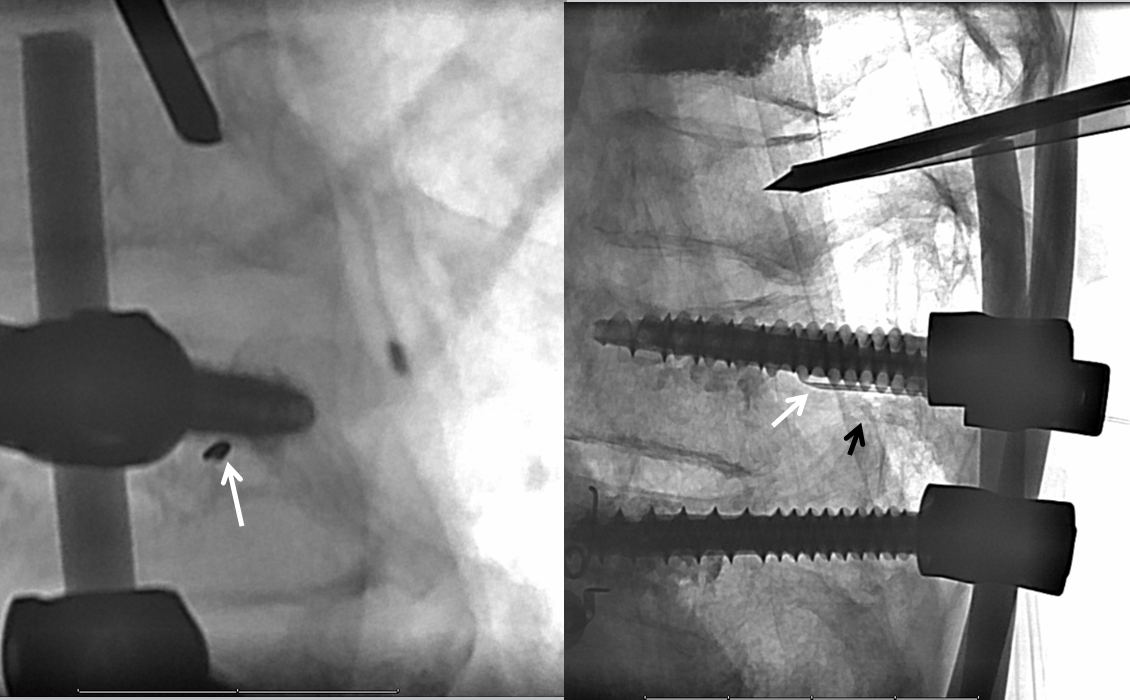
Here is a 14 gauge Spetzler needle going in. The Spetzler works great for this — it is large enough to allow for cement to come out, but much smaller than a kyphoplasty system, which is more like 10 gauge. Look how the needle slides right under the screw.
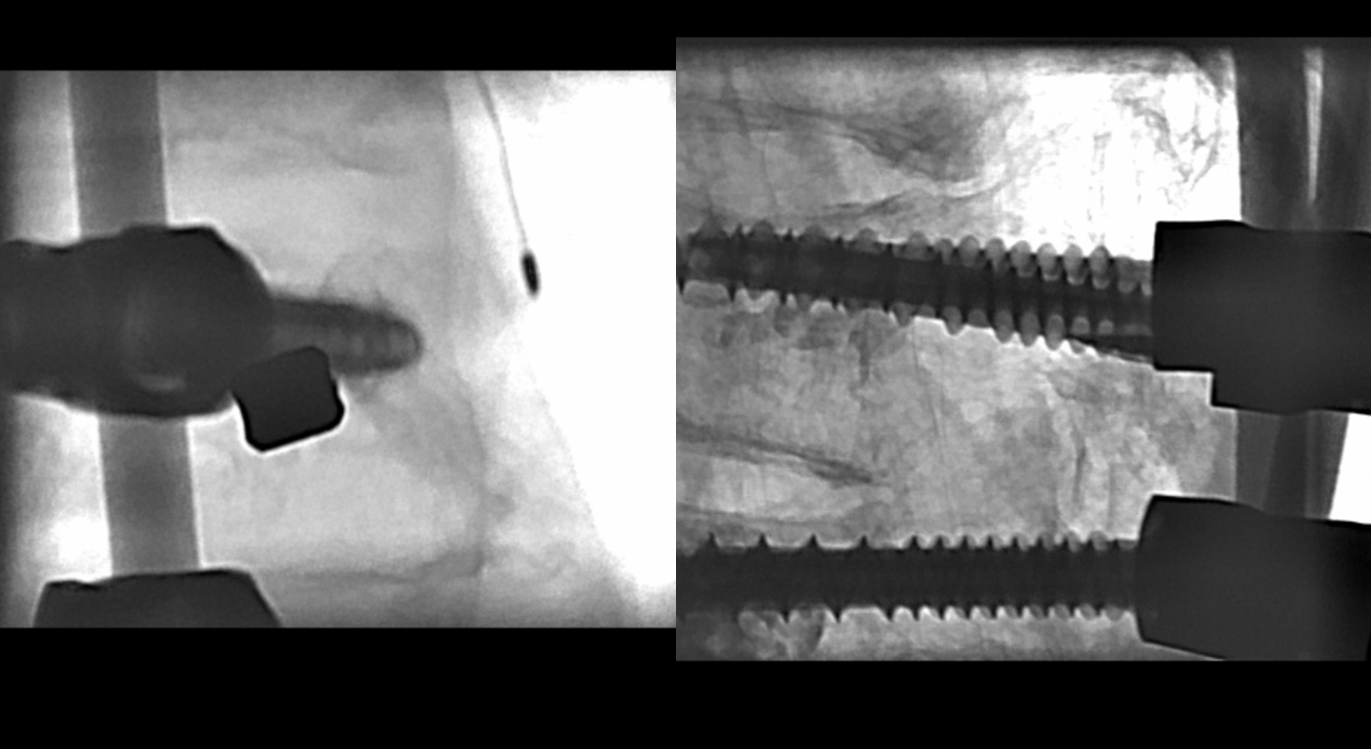
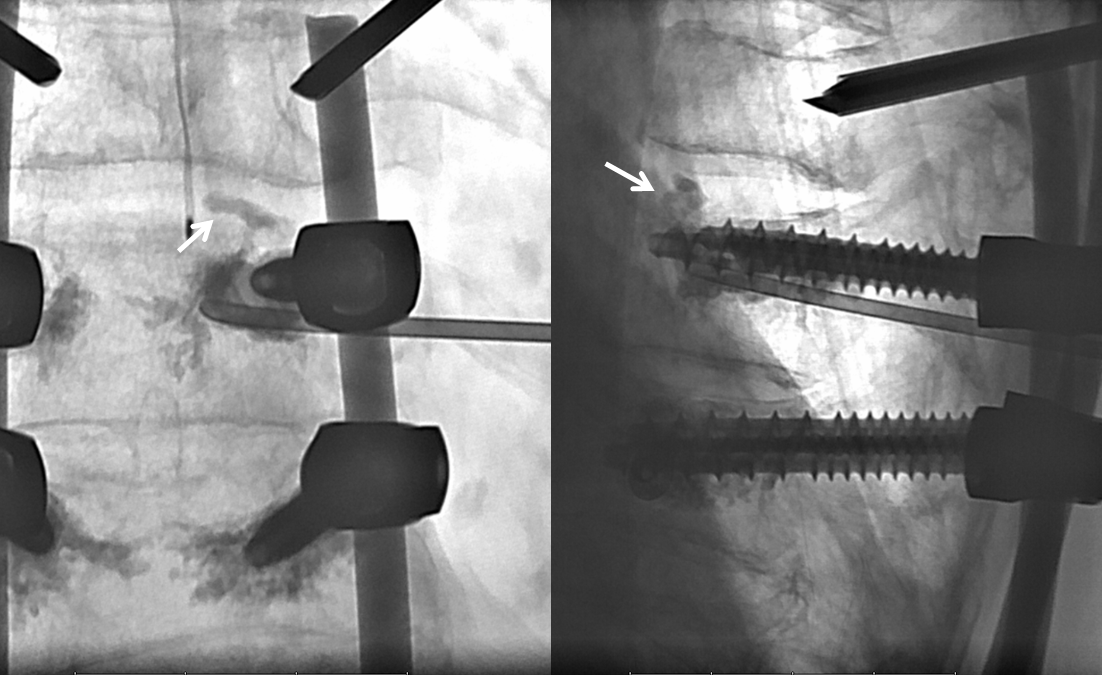
Now we switch to true frontal plane to make sure we do not violate the spinal canal and best gauge the position of the Spetzler needle in the body. Notice lucency around the screw (white arrow). The needle is placed medial to the lucency on purpose — to be able to extrude some cement into the vertebral body trabecular system and anchor the cement which will fill the lucent area around the screw
An oblique view shows the Spetzler needle trajectory under the pedicle. The curved part of the needle can be directed away from the thread, if necessary
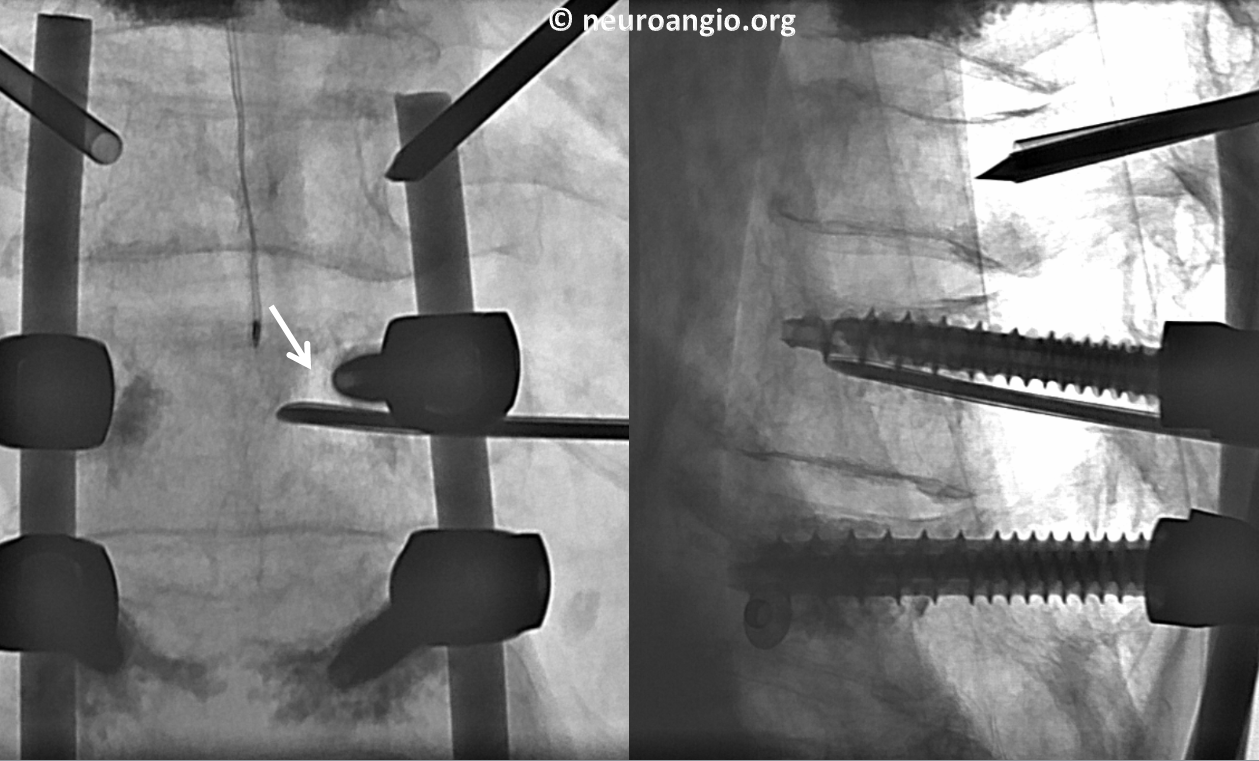
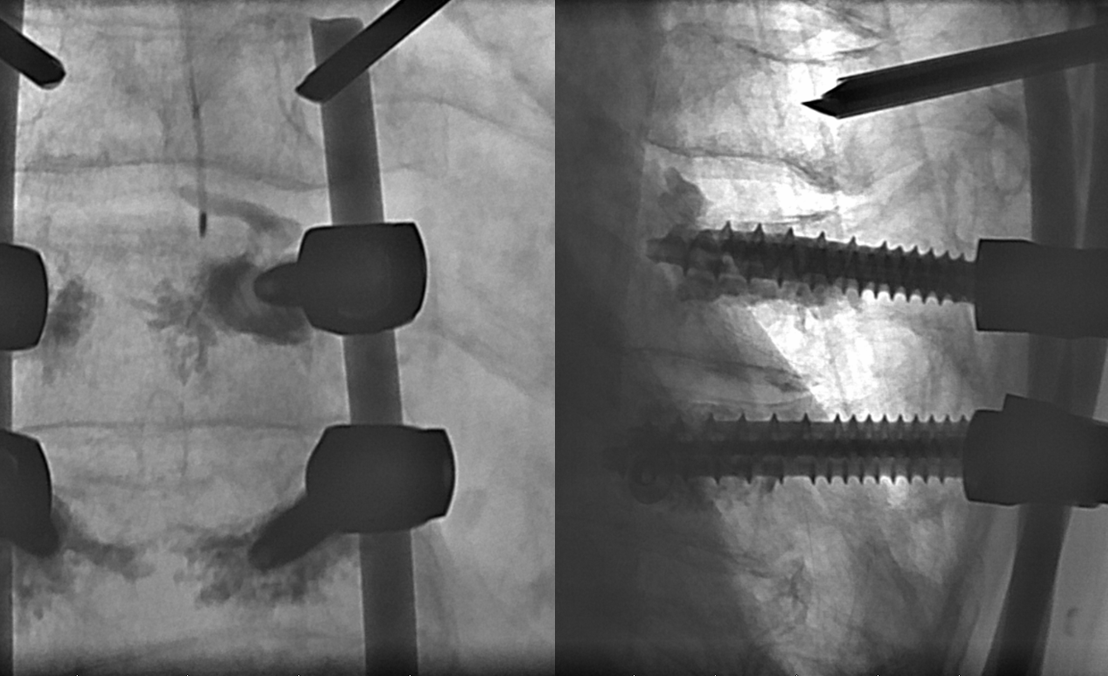
Quick-to-Dough Bone polymethylmethacrylate (PMMA) cement is loaded into 1 cc syringes. If you use older PMMA cement, make sure it is relatively thick. The Quick-to-Dough goes in well through a 1 cc syringe about 5 minutes after start of mix. Only a few minutes of work time are available so make sure you are ready. Biplane angio is super useful here. White arrows show the cement “anchor” in the vertebral body.
Some cement finds a hole in the superior endplate (white arrows). At this point, the stylet is re-introduced while simultaneously withdrawing the Spetzler needle to fill the void created by the needle itself and prevent further cement leak into the disk space
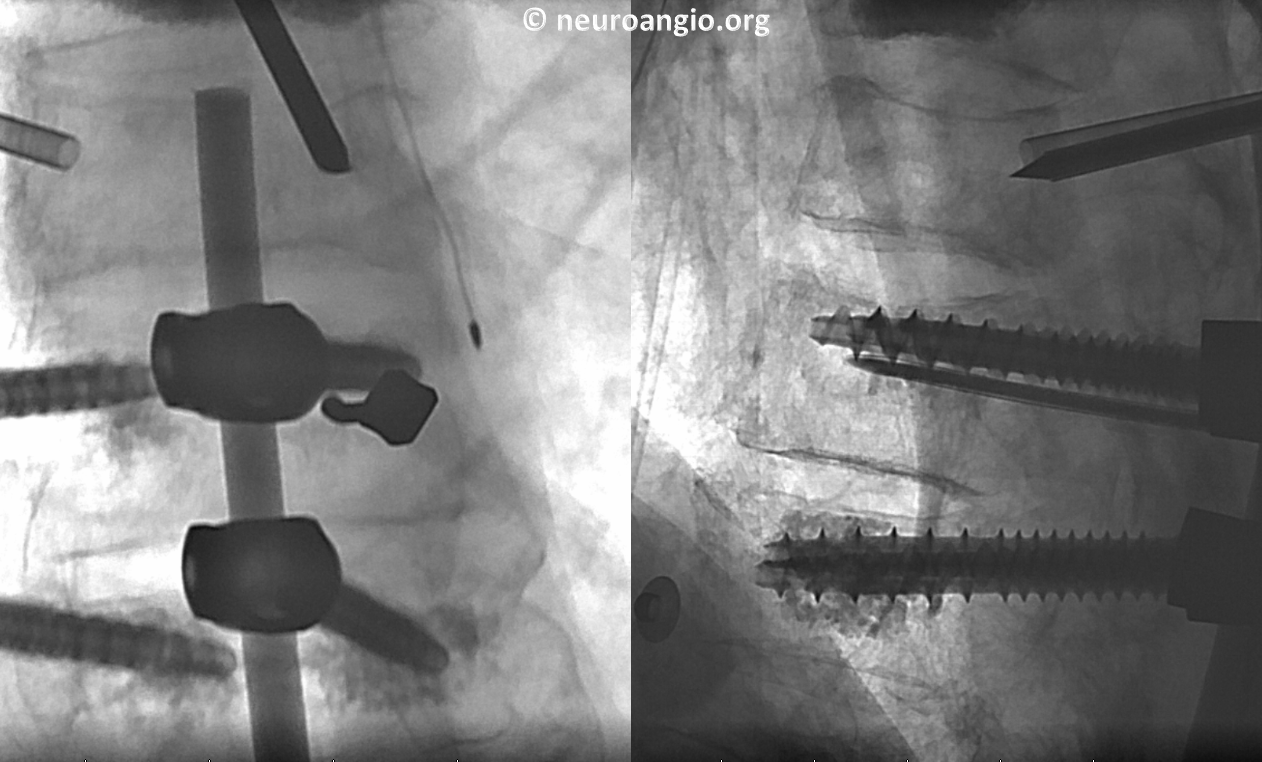
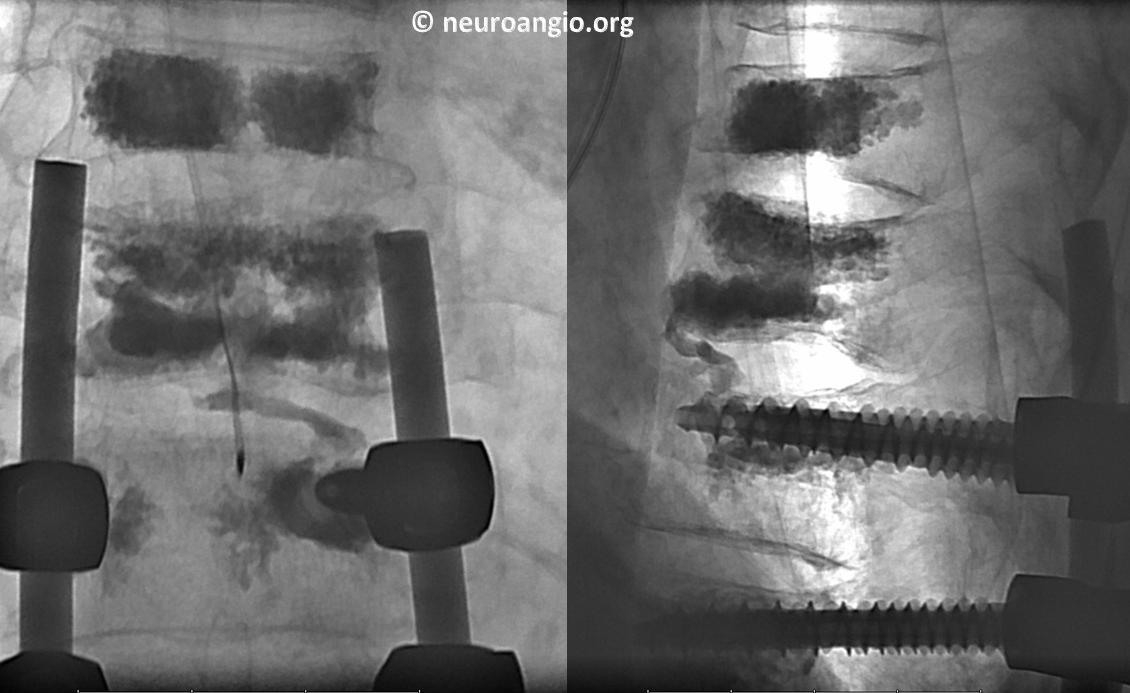
Final. Not bad, right. There is plenty of cement in the vertebral body to anchor the part around the loose screw.
Final picture after T10 kypho. Check out the anterior T10-11 cement fusion (just kidding)
Post-procedure axial CT. Not bad, right
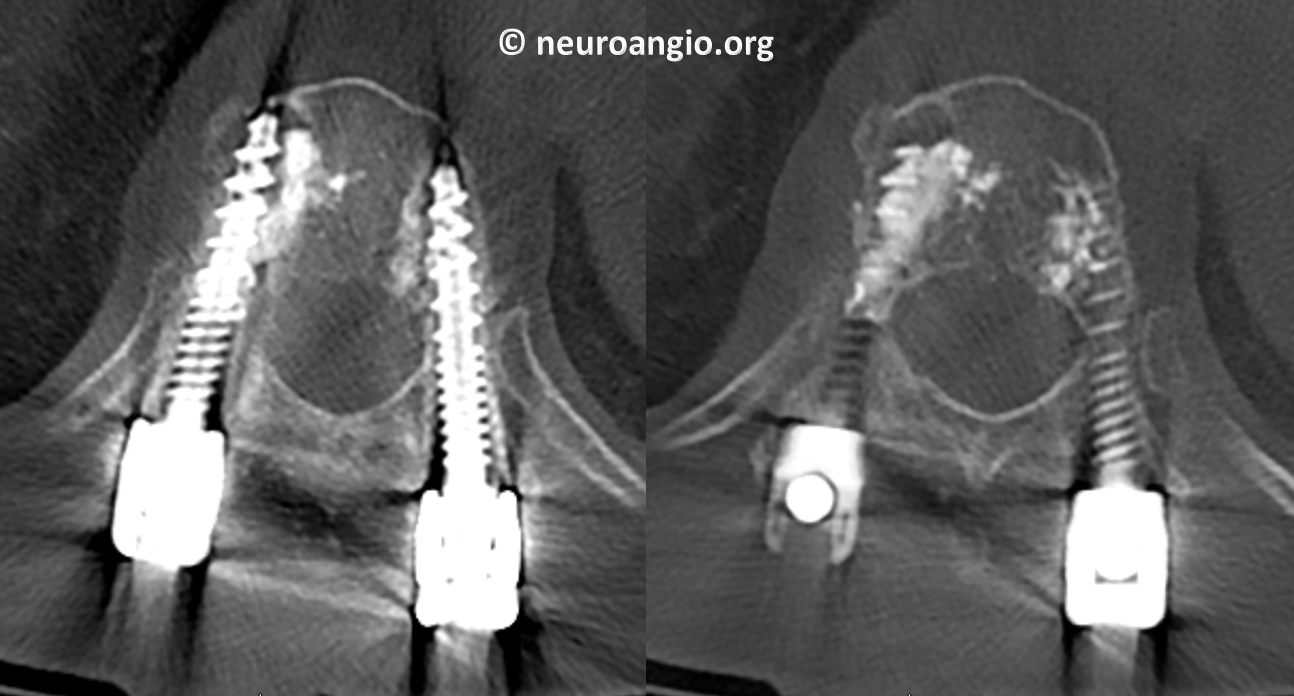
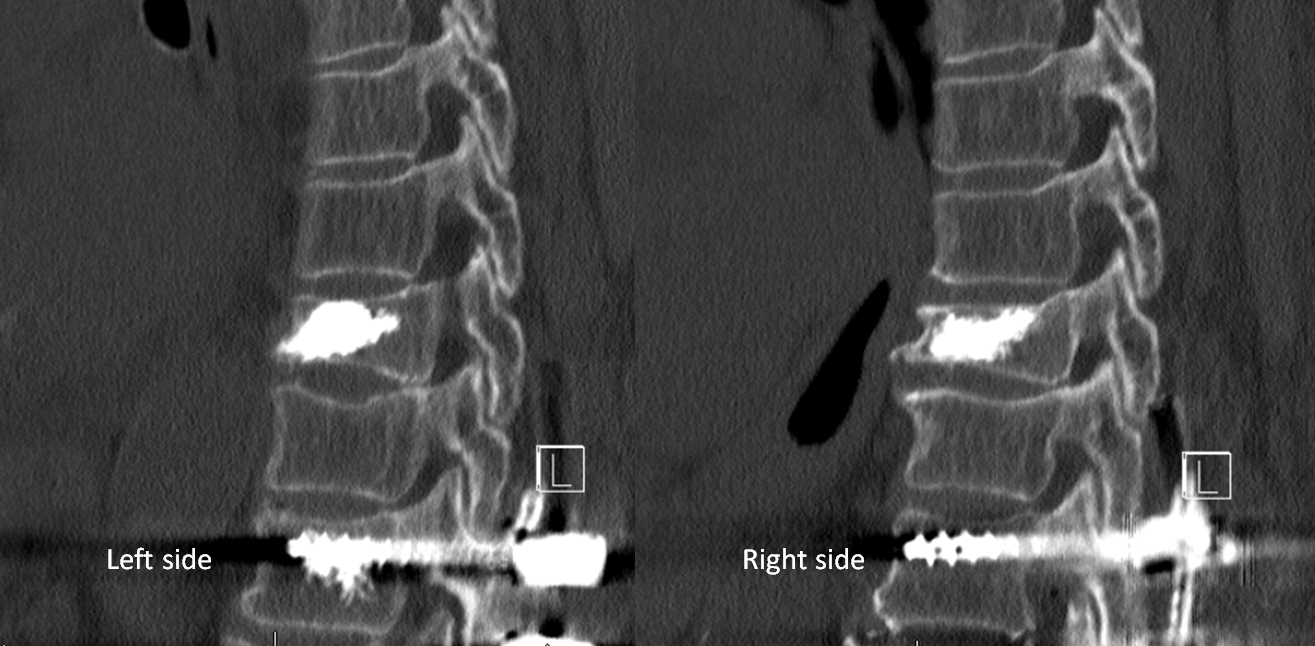
Sagittal and Coronal. The lucency is filled (white arrows) with extension of cement into mid-body (black arrows) to hopefully keep it in place
Questions/comments: Contact the Galaxy’s Best Spine Institute here.