Another example of how understanding vascular anatomy leads to safe and effective intervention.
Case courtesy Drs. Nelson and Tanweer
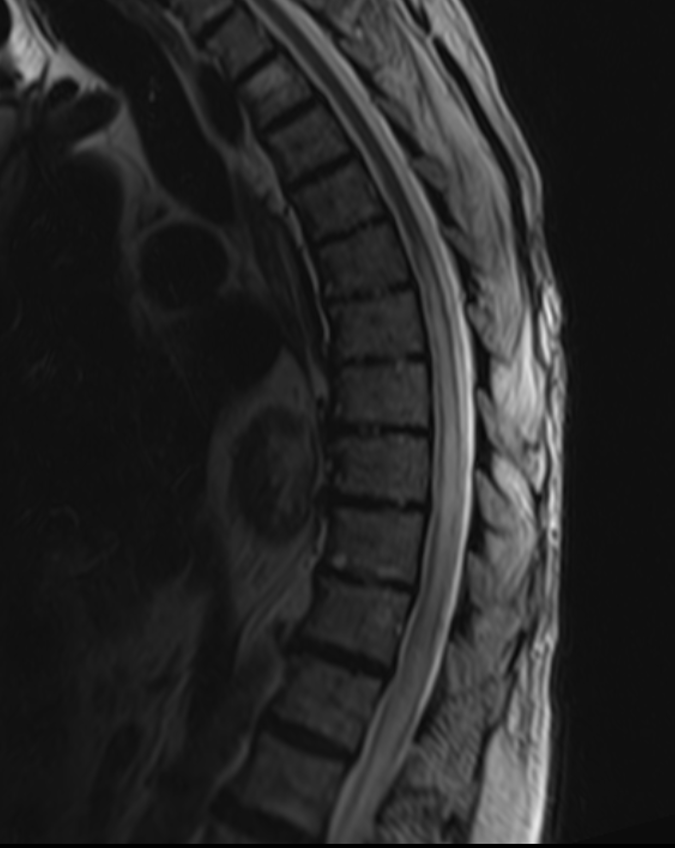
Presentation is with typical progressive myelopathy
Typical MRI
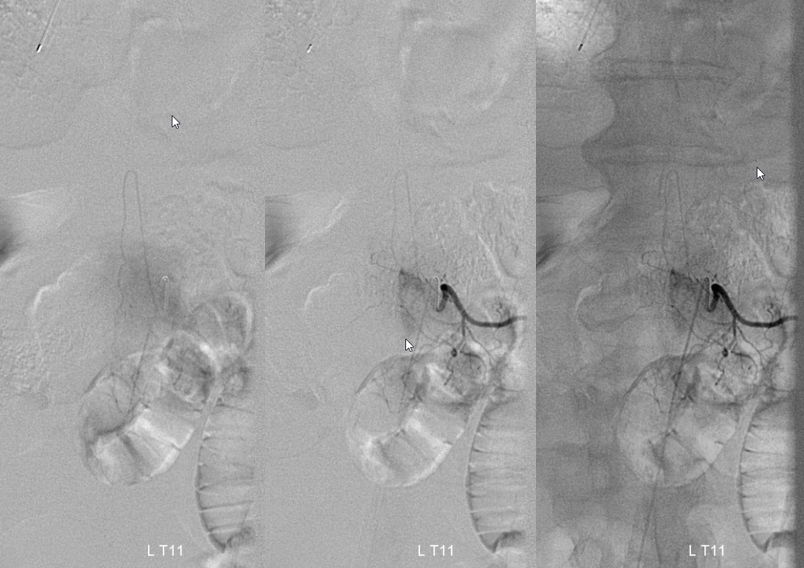
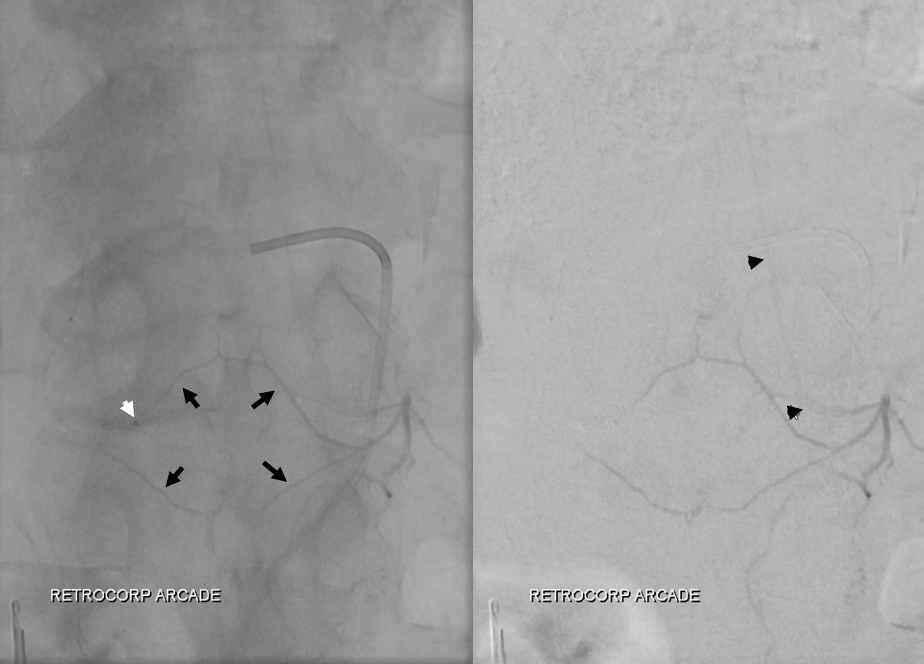
Right T11 origin dural fistula (draining vein = white arrows)

The Adamkiewicz happens to arise from left T11 — just across the river. Too close for comfort. Forget about those random mouse pointers — i’m too lazy to re-image.
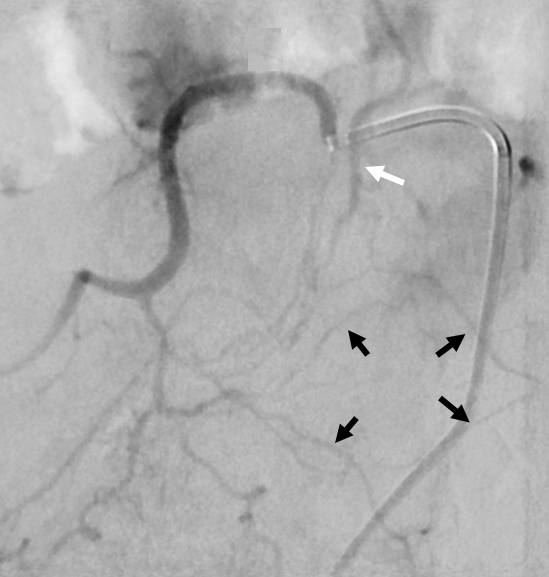
What to do? Get better images. Close-up view of Right T11 shows draining vein of the fistula (white arrow) and the epidural arcade (black arrows). Anatomy knowledge tells us that the epidural arcade is what connects the right and left sides. Thus, the path to the Adamkiewicz lies through this arcade
Here it is. Microcatheter (tip = white arrowhead) is placed into the epidural (retro-corporeal) arcade. Injection shows the arcade (black arrows) and, via this arcade, the radiculomedullary branch (also known as the Adamkiewicz, black arrowheads)
Easy. Block the arcade with some coils (black arrow), and you are in business.

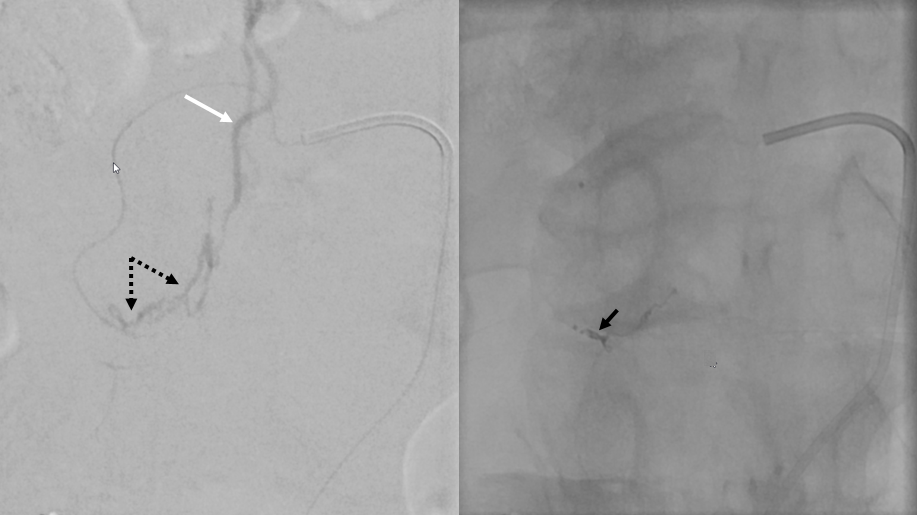
Now, from a more proximal position, injection shows only the fistula (dotted arrows). The path to the Adamkiewicz is blocked with the coils (black arrows)
At this point, a rather unfortunate decision was made to use Onyx, which rarely works for these fistulas. The result is a small Onyx plug, with no fistula permeation.

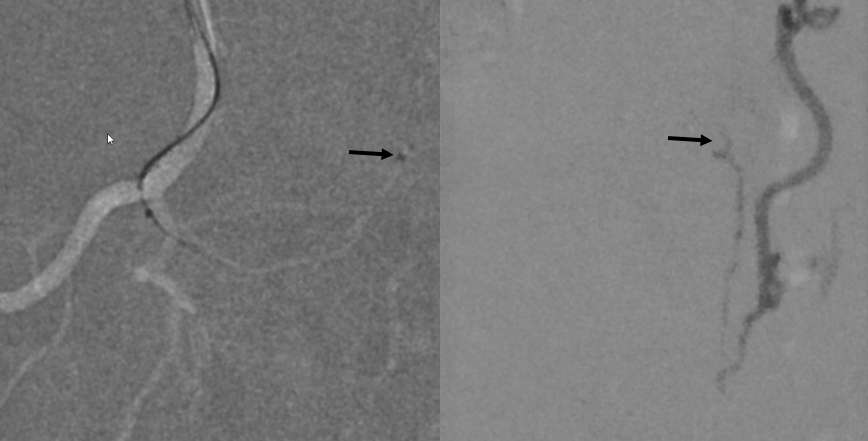
What to do? Again, anatomy comes to rescue. The same retro-corporeal (epidural) arcade that lead to the Adamkiewicz on the other side also allows for fistula access from the level above. Below is injection of right T10 level — showing that the fistula is alive and well (draining vein = white arrows). That’s what happens with proximal embolizations, as we should all know.

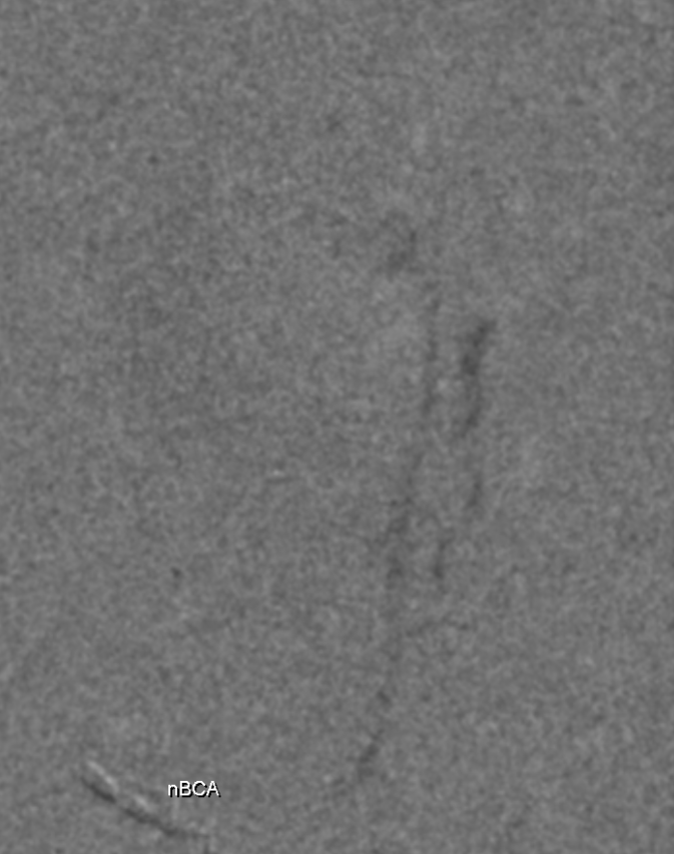
No big deal. We now micro-catheterize the arcade branch leading to the fistula (microcatheter tip = black arrows). The image on right shows the fistula point at the bottom and the same draining vein. The key is to use nBCA.
N-BCA cast show excellent fistula permeation
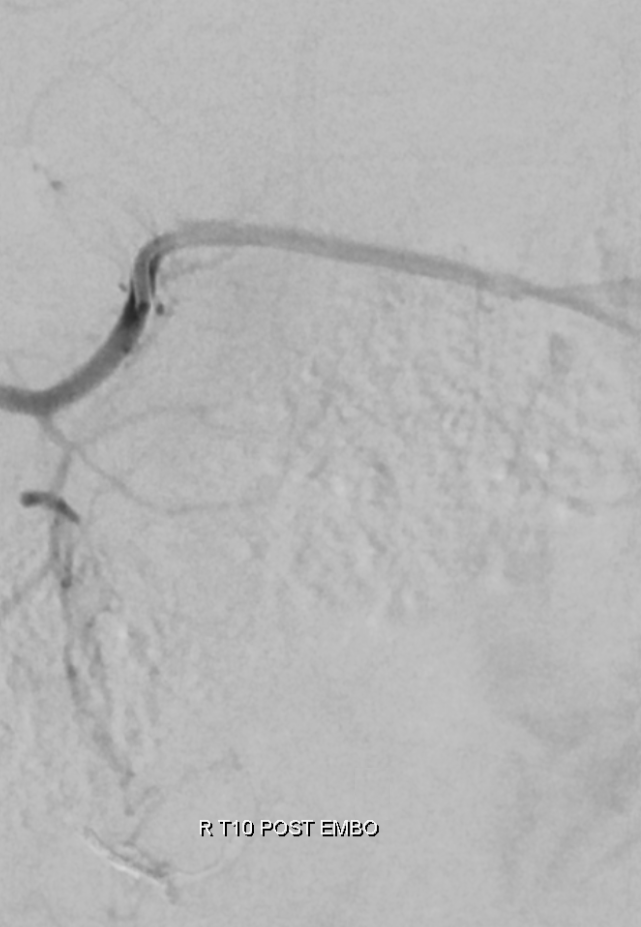
Post-embo Rt T10
Post-embo left T11 — the Adamkiewicz is safe and sound

Not hard at all if you know the anatomy.
See companion case of Dural Fistula Embolization from SAME exact level as the Adamkiewicz.
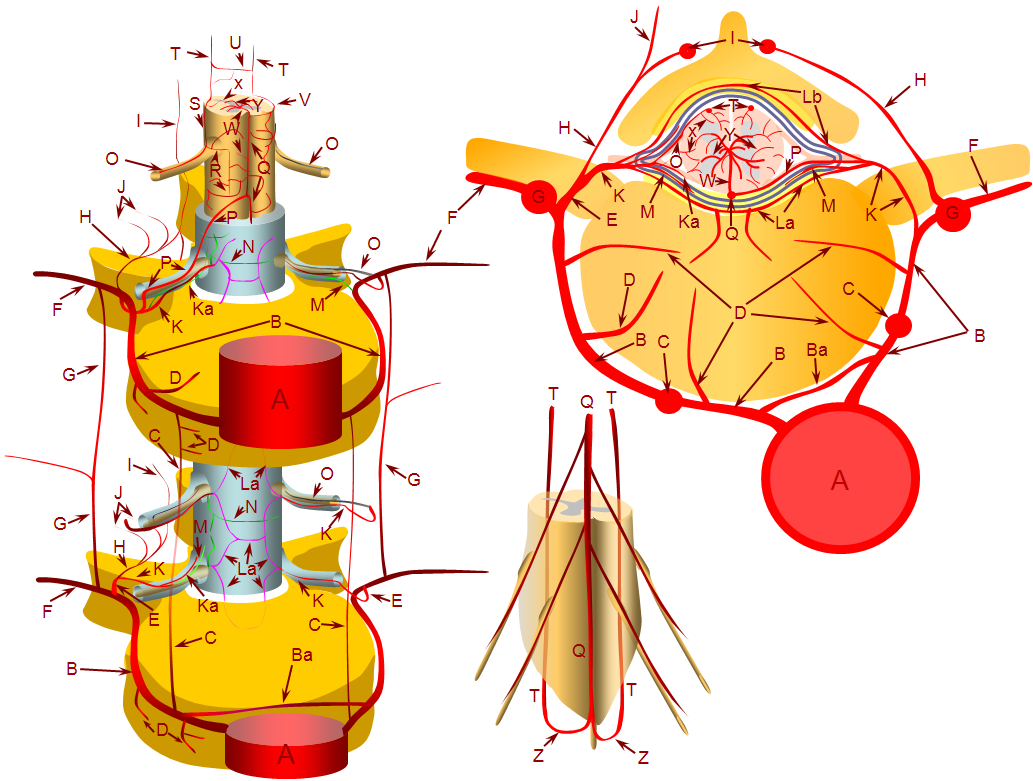
Also see Spinal Arterial Anatomy page for rich background info (like this image below)