
See SPINAL ARTERIAL ANEURYSM page for more info about this condition. This case is a nice example of how easy it can be to miss a spinal aneurysm even on an angiogram, leading to diagnosis of “cryptogenic spinal hemorrhage”
Superb detective neurointerventional work by Dr. Eytan Raz who reviewed these outside images, which were read as “negative”, to make the correct diagnosis.
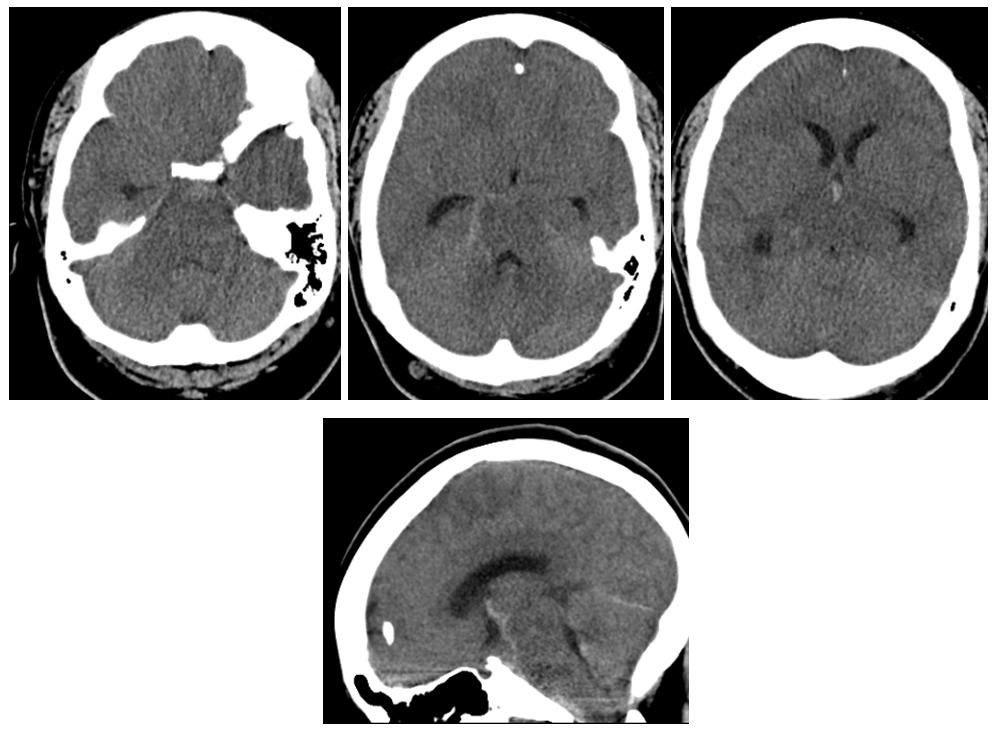
The patient presents with headache followed by back pain and paresis. CT shows subarachnoid hemorrhage in the posterior fossa
MRI shows what should have been recognized as a spinal aneurysm at T6/T7 level

Lateral shows aneurysm on left side of cord at same T6/7

These images, in our opinion, are pretty much diagnostic. At least extremely highly suspicious. Angiogram is done at “outside institution”
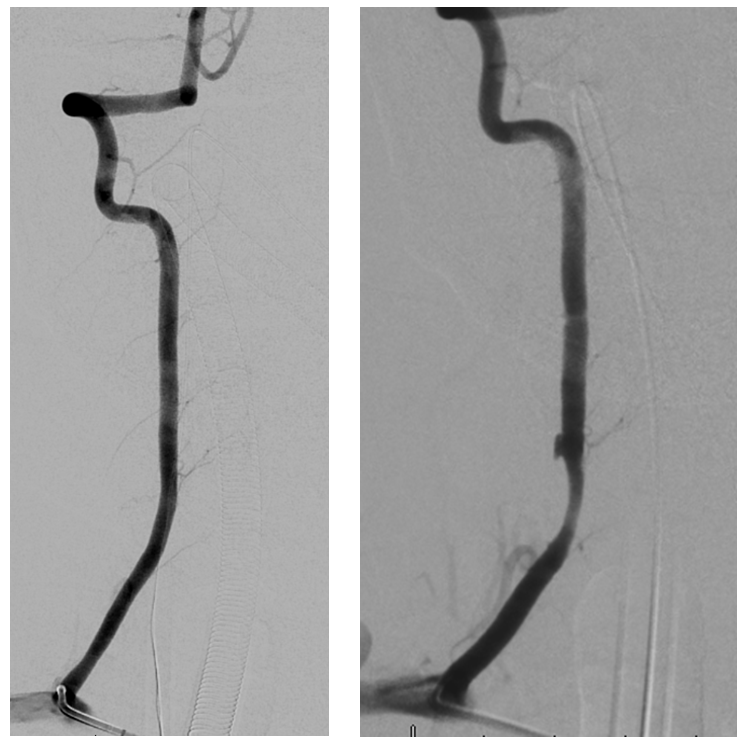
Vert dissection, just like case 1 on Spinal Arterial Aneurysm page
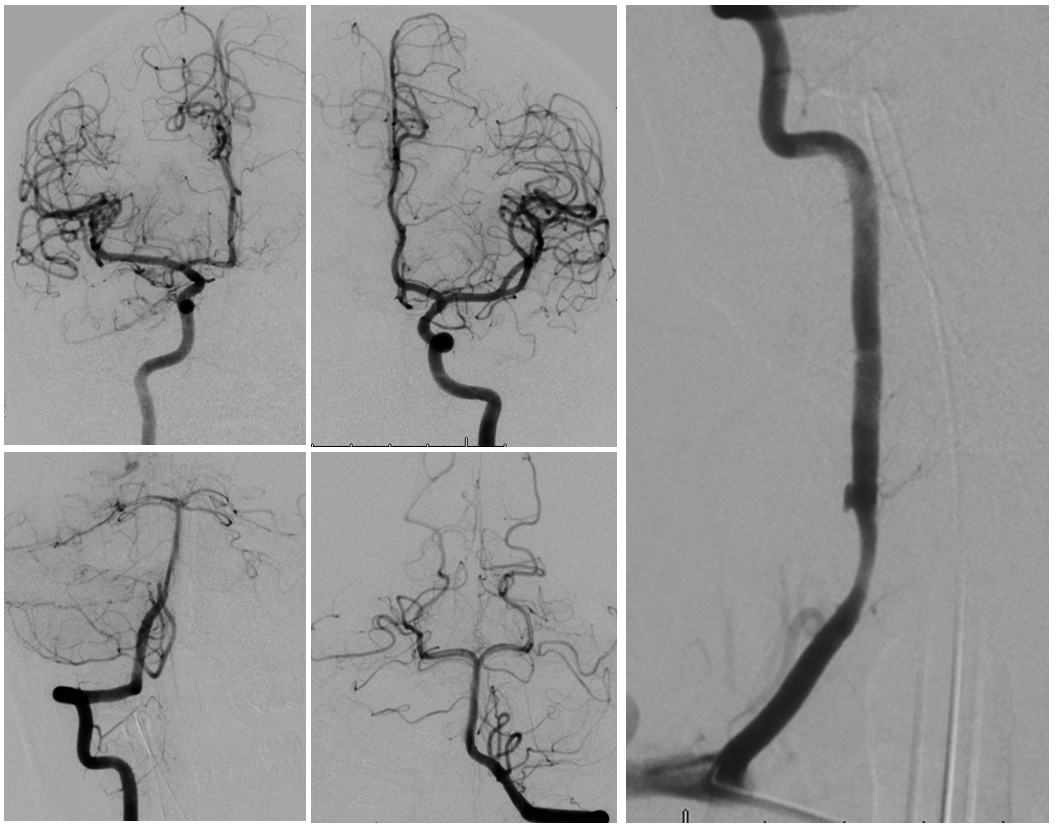
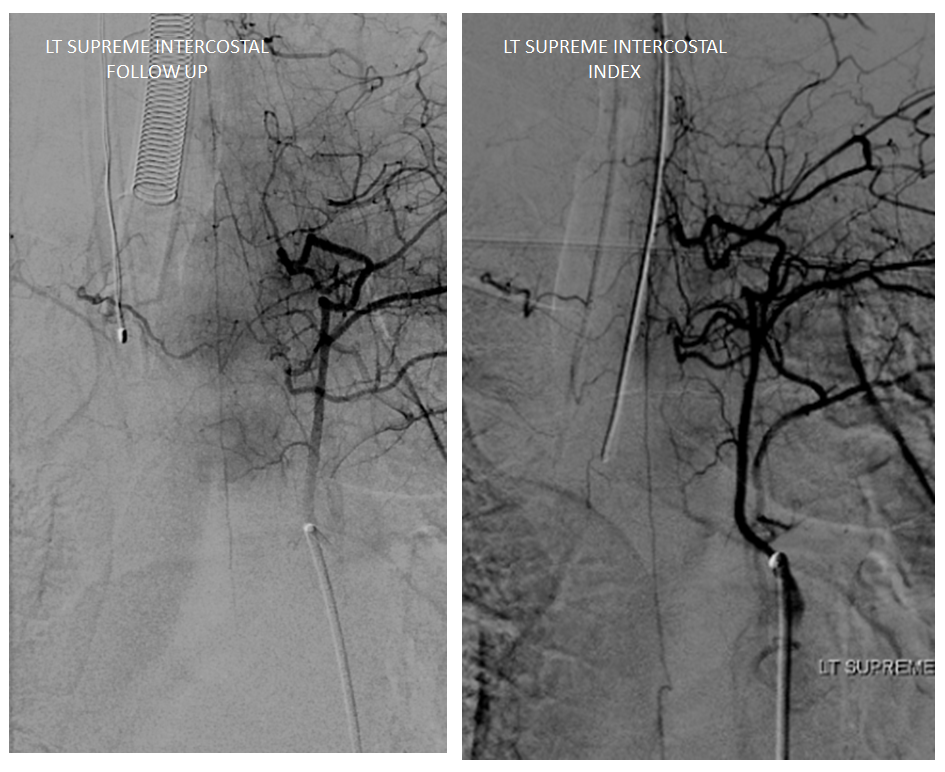
Radiculomedullary supply to entire thoracic cord is from left supreme intercostal
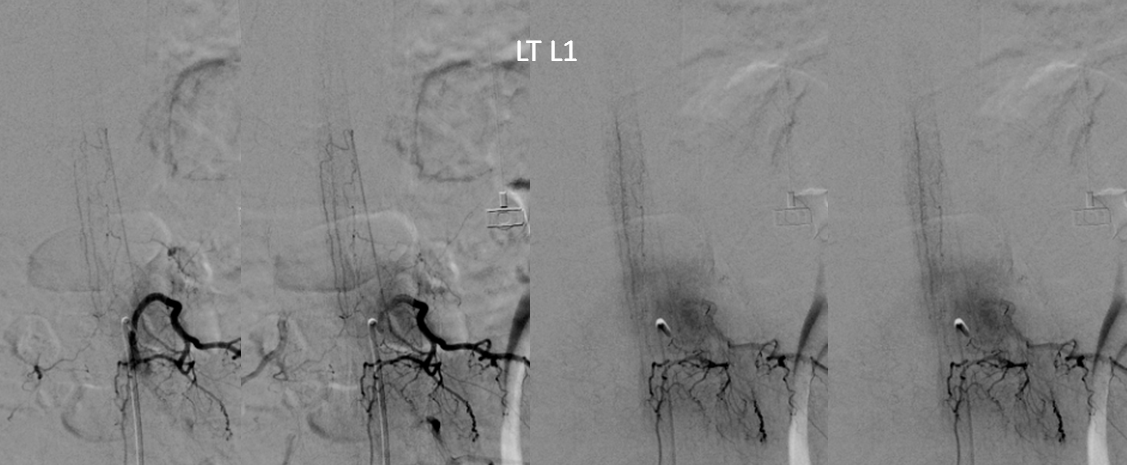
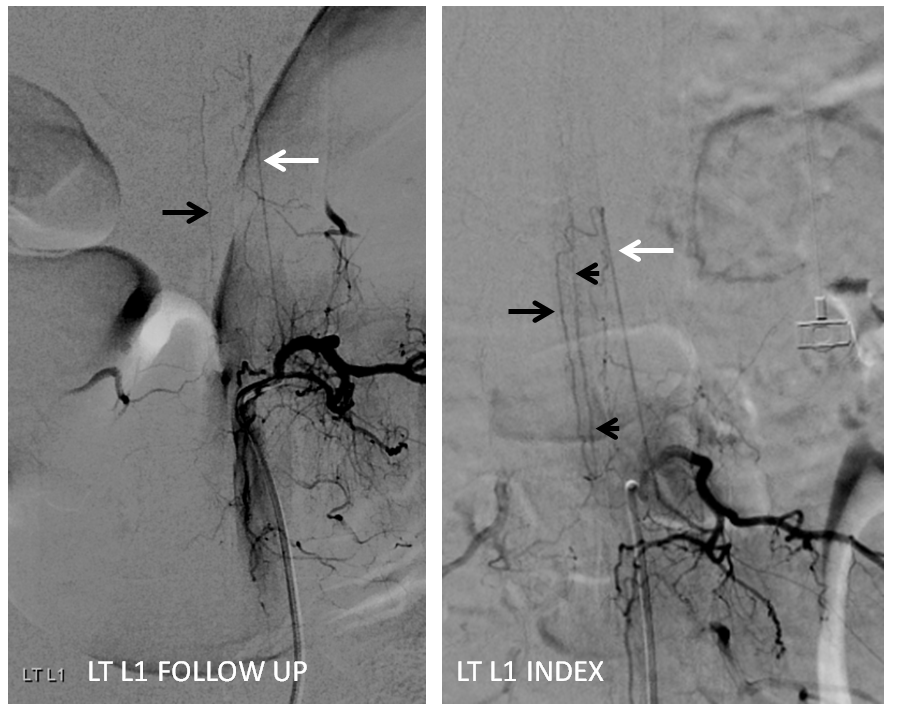
At conus supply is from left L1
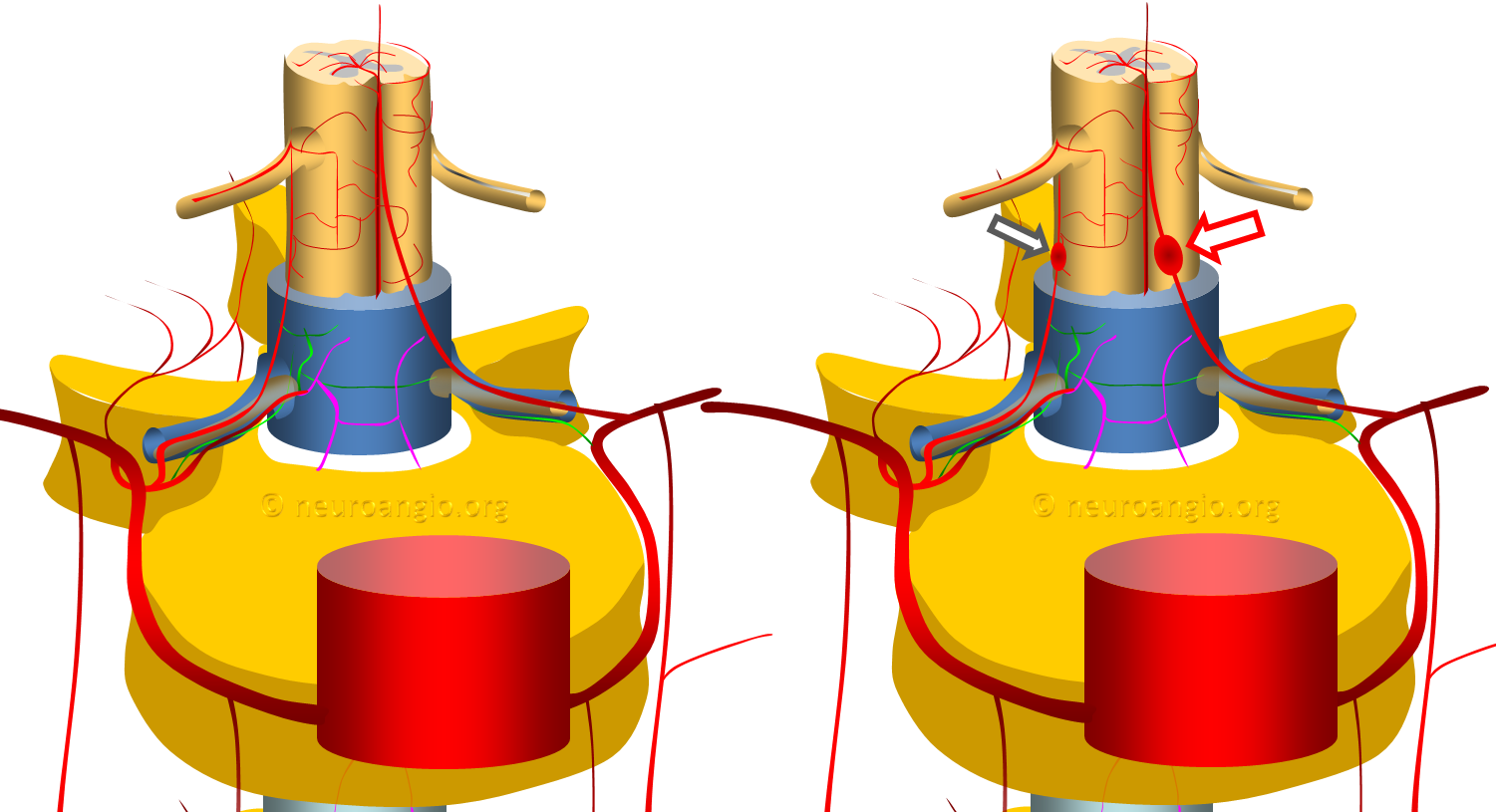
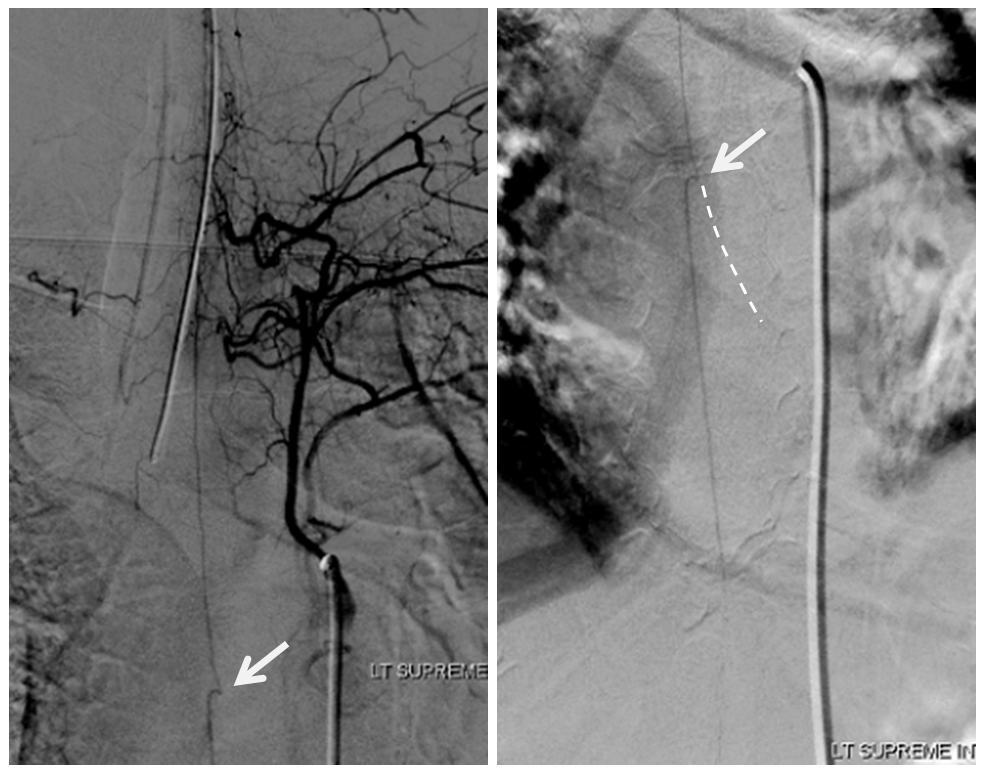
Angio is read as negative. It is not. An experienced operator will notice a few highly unusual things. First, there is no “Adamkiewicz”. Supply to nearly all of cord from as high as supreme intercostal is extremely unusual. Also, there is a characteristic “kink” at the mid-thoracic level of the ASA (arrow below) just at the midthoracic level, where aneurysm is suspected on MRI. This kink shows location of another radiculomedullary artery contributor. The presumed nonvisualized vessel is shown with dashed white lines
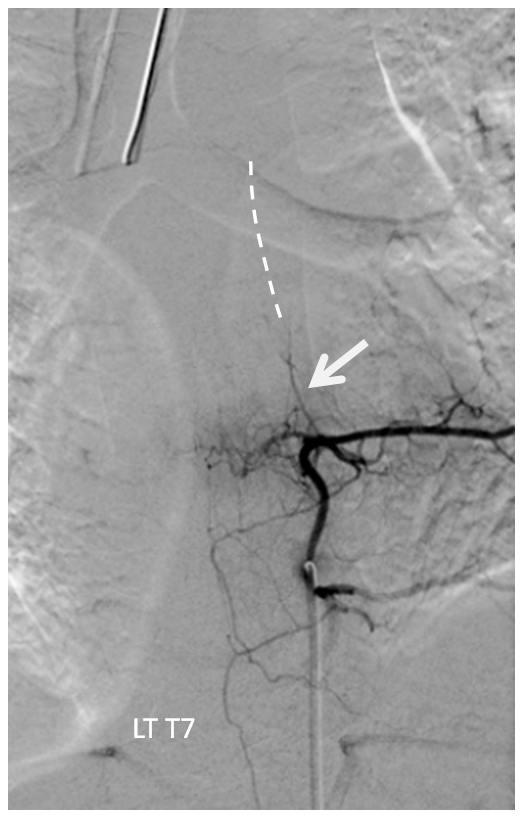
A look at left T7 segmental artery shows an unusual vessel (arrow) that resembles a proximal radiculomedullary artery, the presumed continuation of which is shown in dashed lines
Finally, the anterior spinal artery at the conus level is supplied in retrograde fashion by the posterior spinal artery (image below, not labeled. There is an image even lower done which explains it. Take a look). This is distinctly abnormal. It should be the other way around.
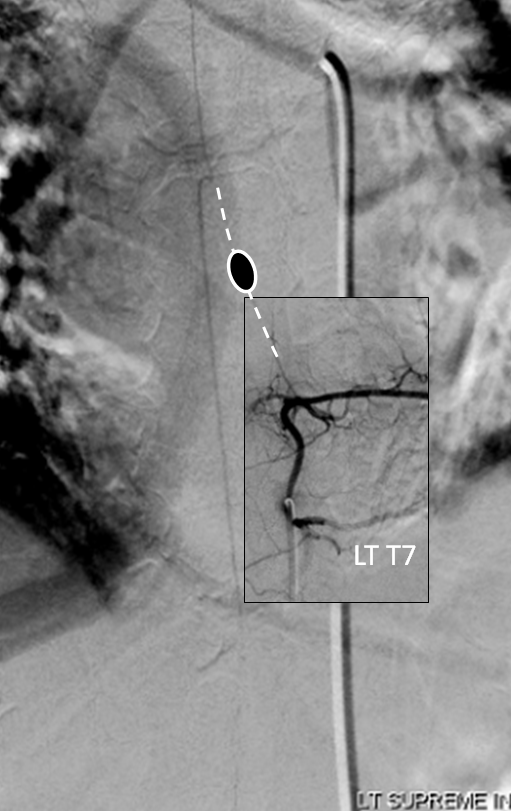
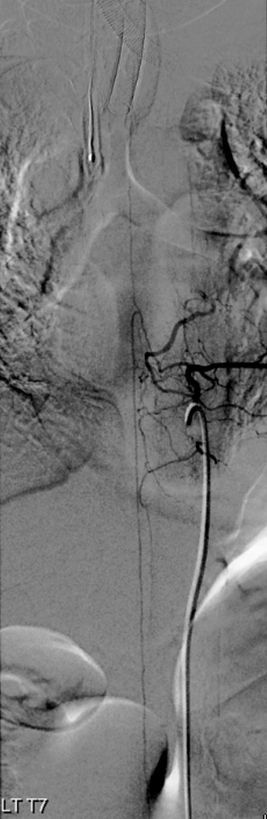
The conclusion is that an aneurysm must have been present at the left T7 radiculomedullary artery, which is the missing “Adamkiewicz”, as shown in image below, superimposing the supreme intercostal and left T7 injections with missing portion of Adamkiewicz and aneurysm drawn in.
The aneurysm and the Adamkiewicz have thrombosed. Fortunately, there is enough collateral supply between the Supreme Intercostal and Left L1 posterior spinal to allow for cord perfusion.
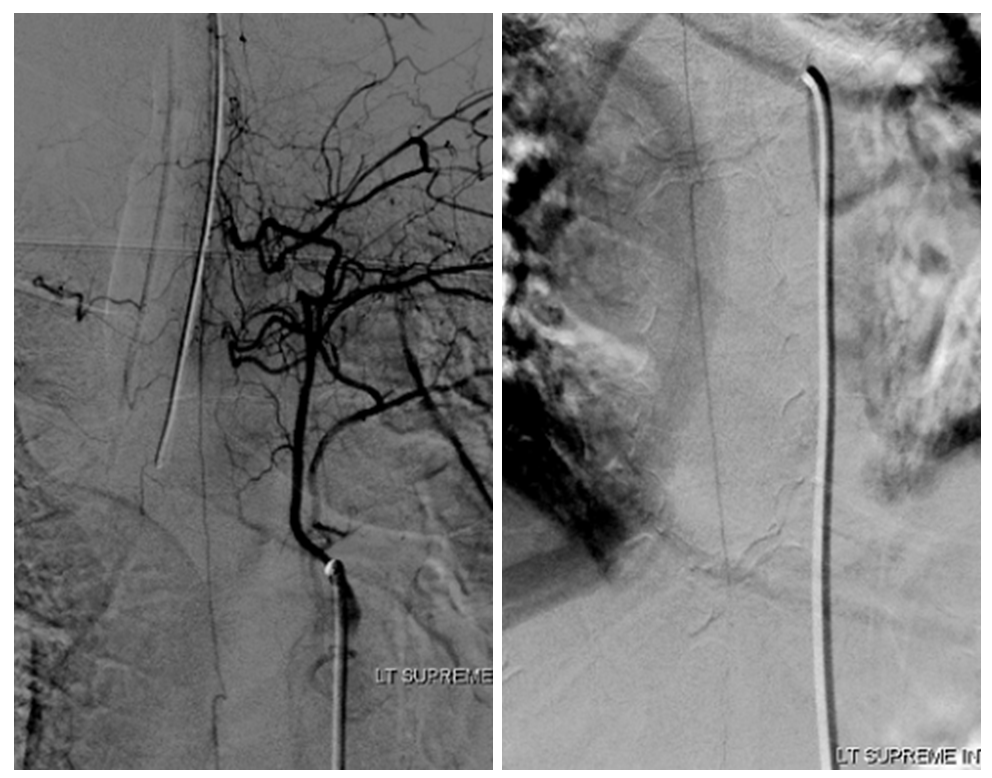
Based on review of above, the patient is brought back for follow up angiography. Look at images below. The supreme intercostal is now supplying a lot less cord (as it should)
The left T7 Adamkiewicz has now recanalized and resumed its contribution to the supply of lower thoracic ASA. The aneurysm is gone. Notice the subtle but highly unusual tortuosity of the intradural Adamkiewicz (white arrow). This artery is never, ever wavy, even in the most atherosclerotic bodies. The tortuous appearance is sequela of recanalized radiculomedullary artery dissection.

Stereo pairs (cross-eye)
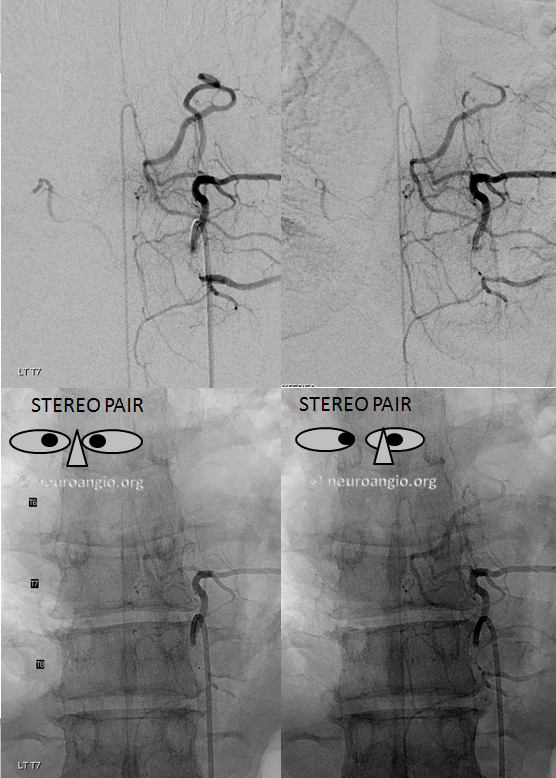

Full length of recanalized Adamkiewicz supply
Left L1 now shows typical relatively prominent posterior spinal artery (black arrow) of the conus, supplied by left L1 radiculopial artery (white). Previously, the same arcade contributed to retrograde supply of the distal anterior spinal artery (black arrowheads)
 q
q
The vert has also healed
Conclusion: Spinal aneurysms can be missed even on angio. Keep a sharp eye and believe your MRI . See Spinal Arterial Aneurysm page for more info
. See Spinal Arterial Aneurysm page for more info