
Case done with Dr. Eytan Raz
The range of interventional options available via upper extremity access continues to expand. Radial is the most common route by far. However, ulnar artery is also a viable choice. When bigger than radial it can also be used.
Now, a few things to keep in mind
1. Ulnar access is more technically challenging — the artery is deeper and does not have the same bone support underneath that the radial artery does. It rolls more. So, unless you are a real expert, ultrasound guidance is mandatory. Do not try it without ultrasound.
2. The ulnar nerve is lateral to the ulnar artery. Just like in the groin. So, try to stay midline or medial
Whether radial or ulnar, a 6F sheath allows for possibility of double catheter use — balloon-assisted coiling for example
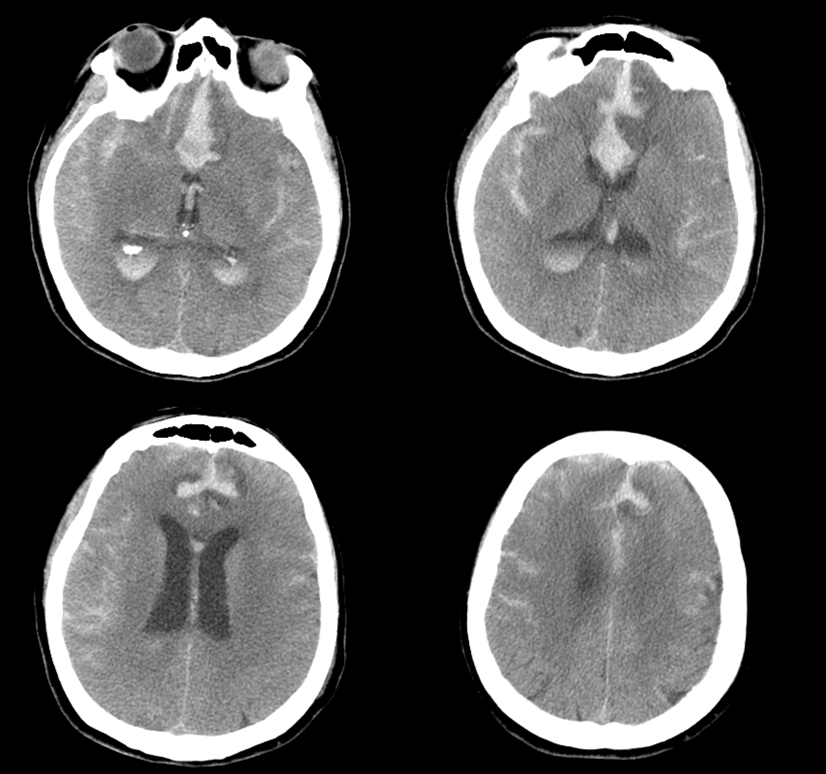
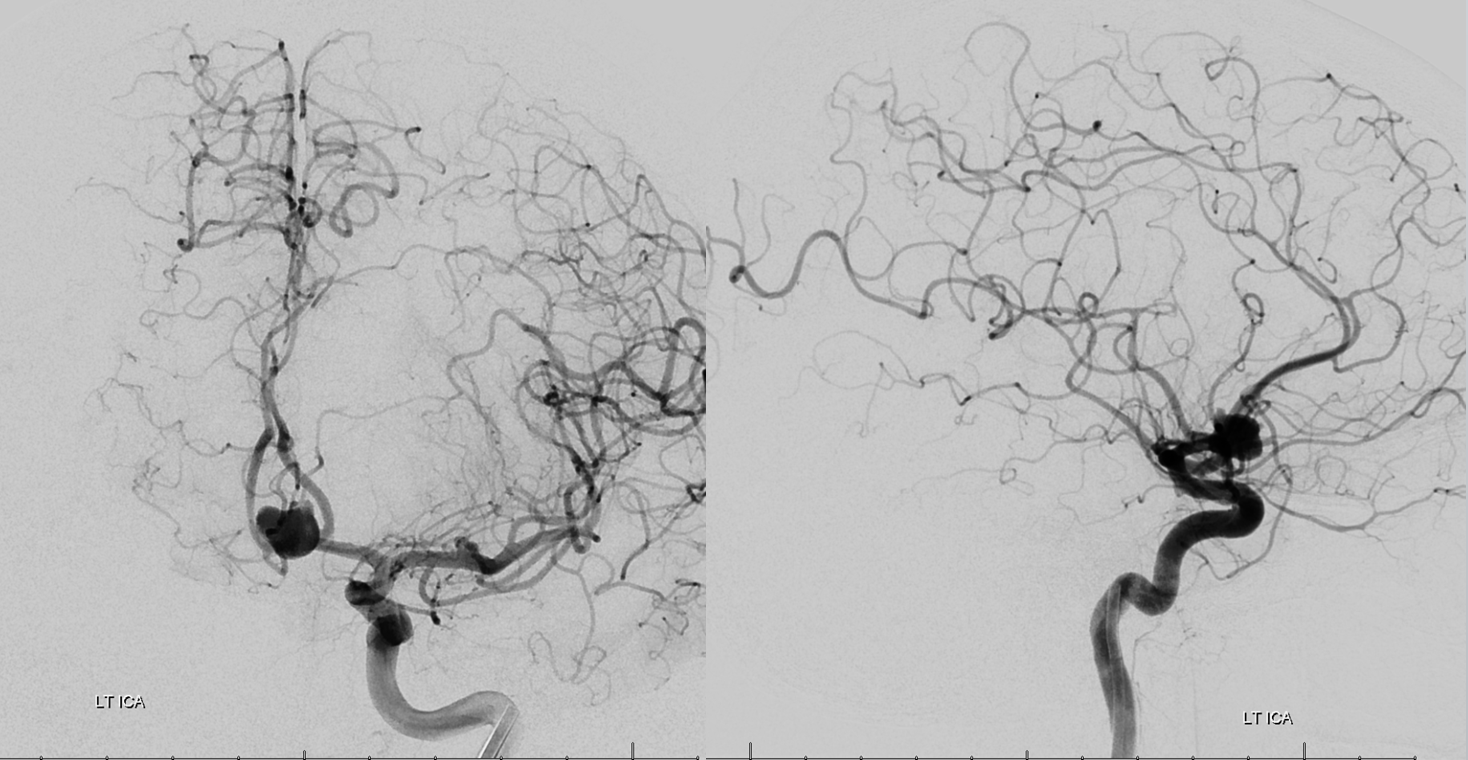
In this case of a ruptured anterior communicating artery aneurysm, supplied via a dominant left A1 segment, is coiled via ulnar access with balloon protection. We ended up keeping the balloon in the supraclinoid carotid in case we ruptured and had to have some kind of flow control, as the right A1 was hypoplastic. Thankfully we never needed to use it. But, it is possible to have it with arm access and, in any case, we prefer a 6F guide in the left carotid when doing radial or ulnar — much more support than 5F systems.
4F vert

No A1 seen from here
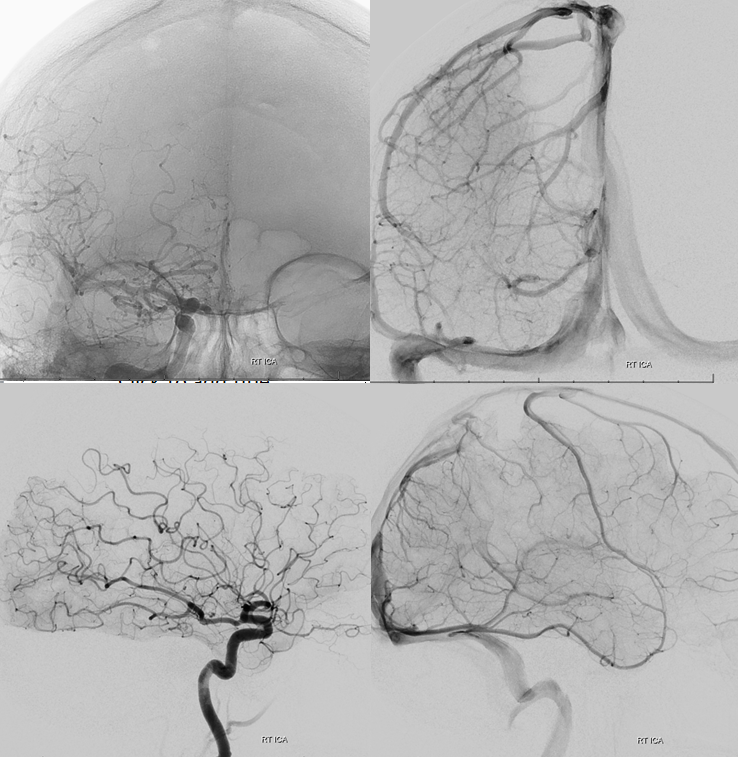
How about this ima? Superior access route 🙂

5F Simmons 2 for the left CCA
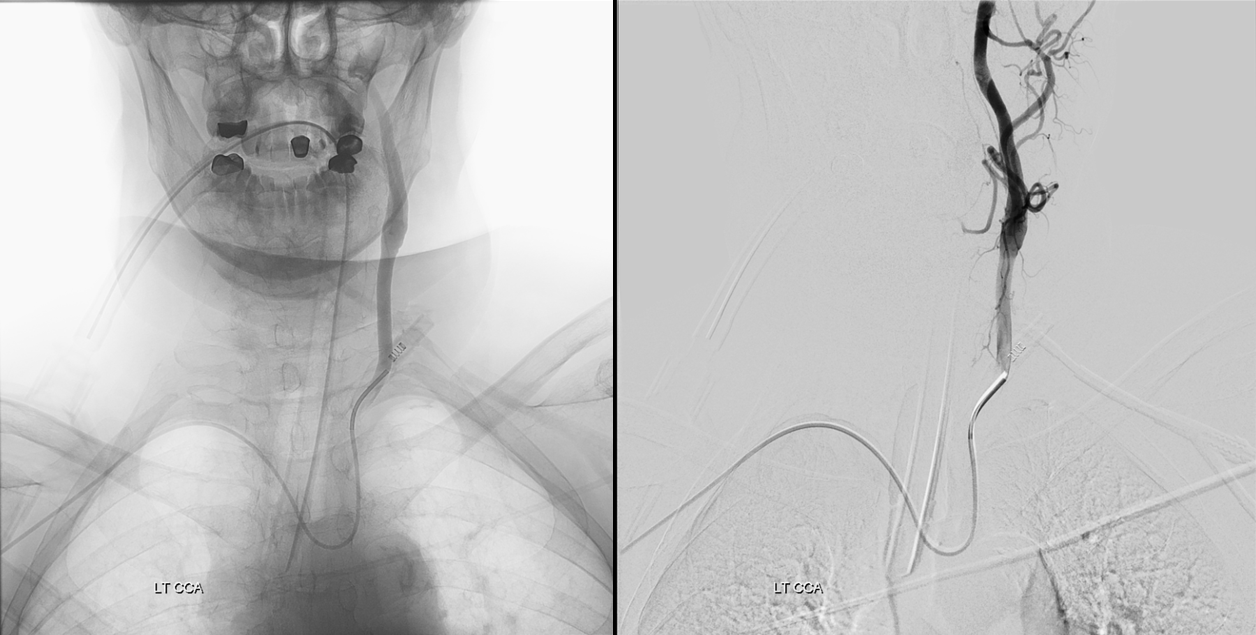
Exchanged for 6F Envoy. It is essential to place the guide as high as safely possible into the carotid. Too low a position leads to loss of support during catheterization
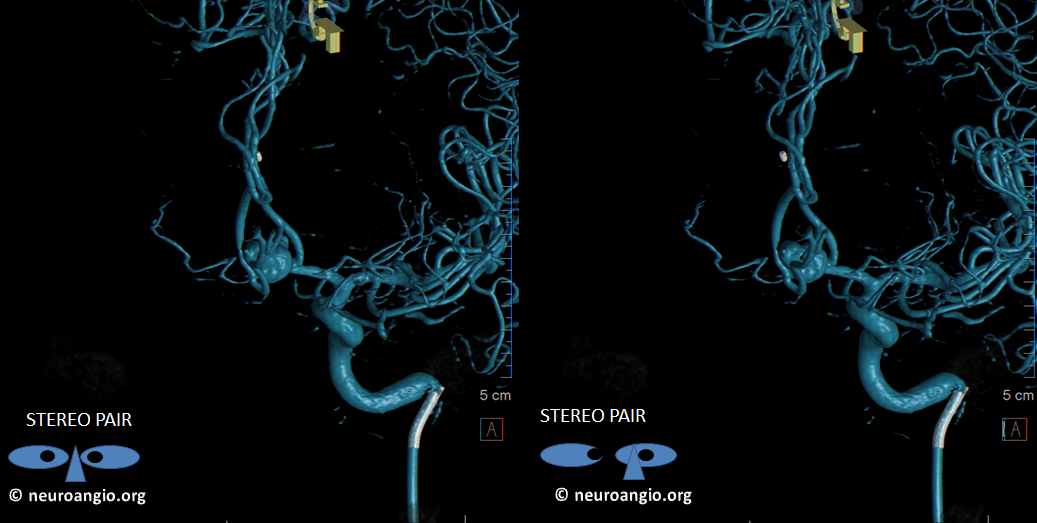
Volumetric views show a multiloped wide neck ACOM. There is no way to coil this completely. Surgery was not pursued due to advanced age and feasibility of subsequent Pipeline treatment
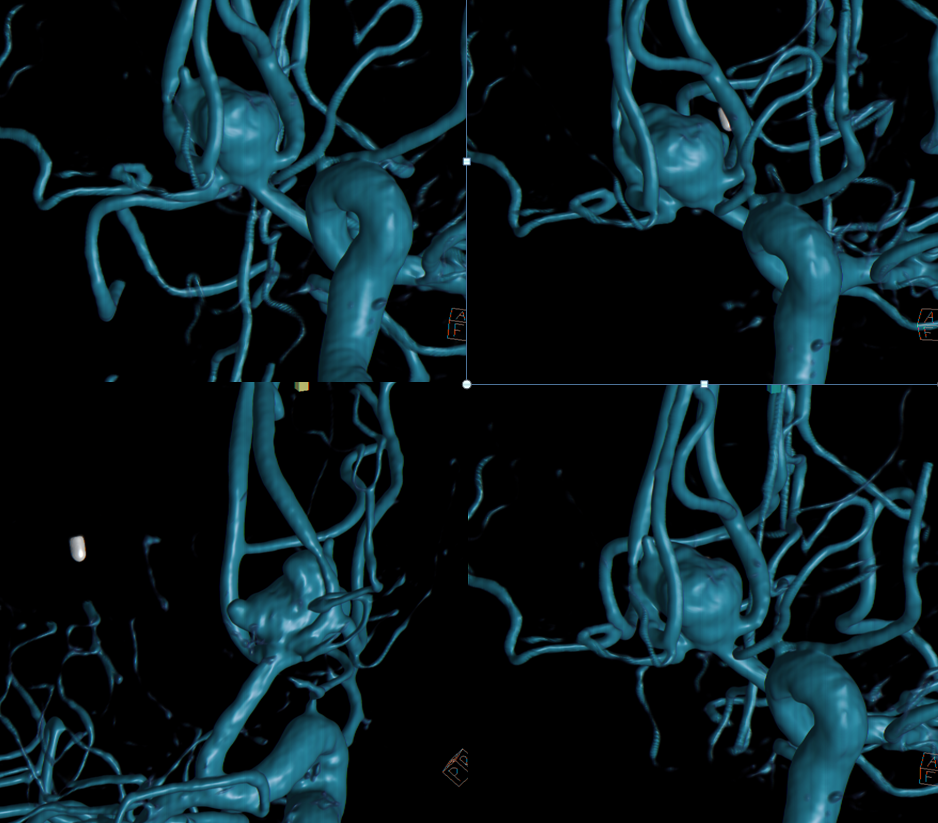
Stereo views
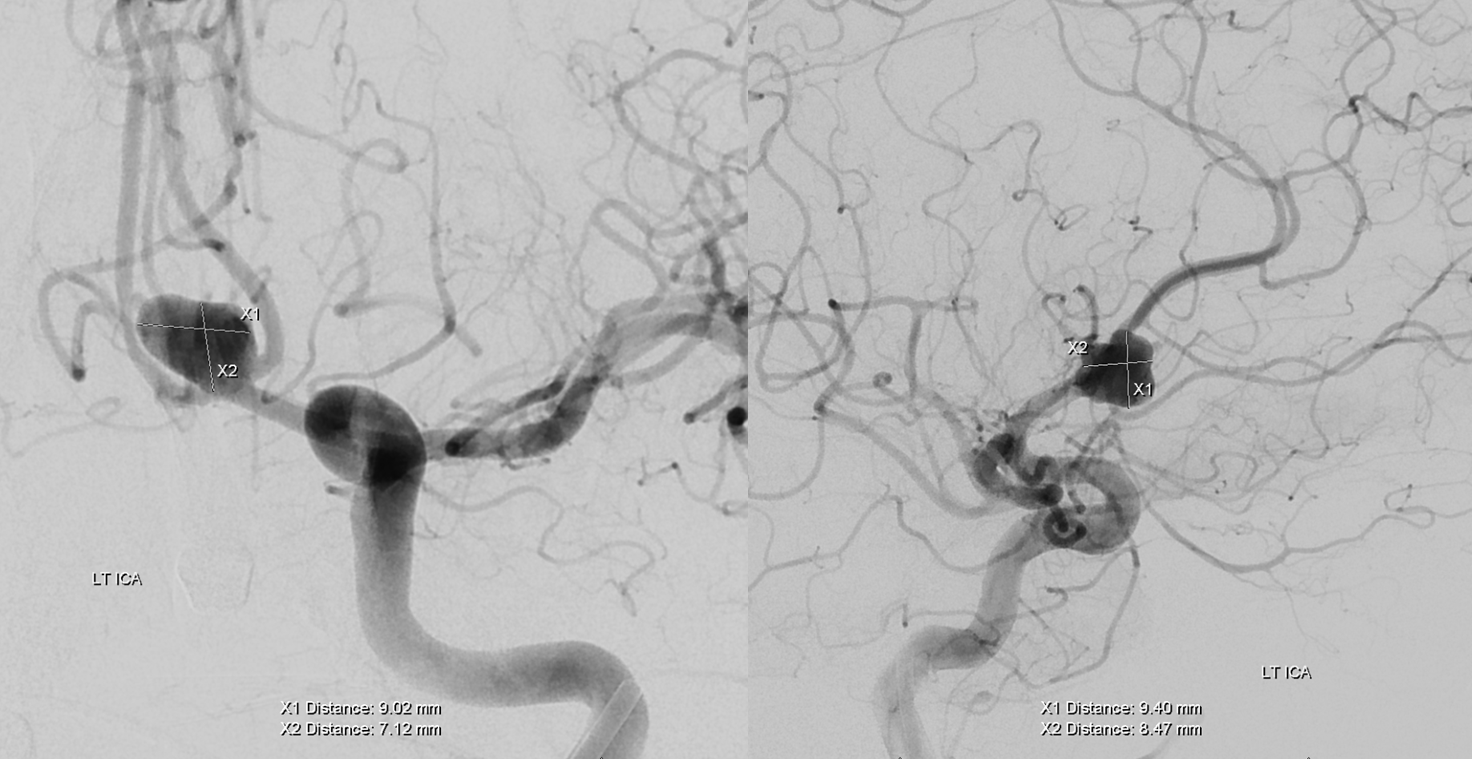
Working projections
First coil — a 6×30 Stryker 360 XL worked out, after a ton or repositioning. Deflated balloon is ready in the supraclinoid carotid (white arrows)
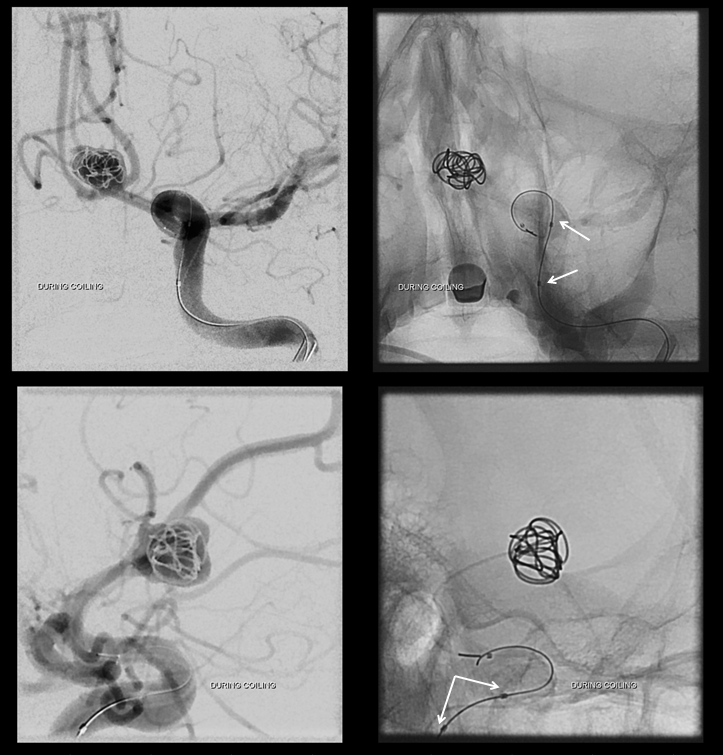
Progressive coiling
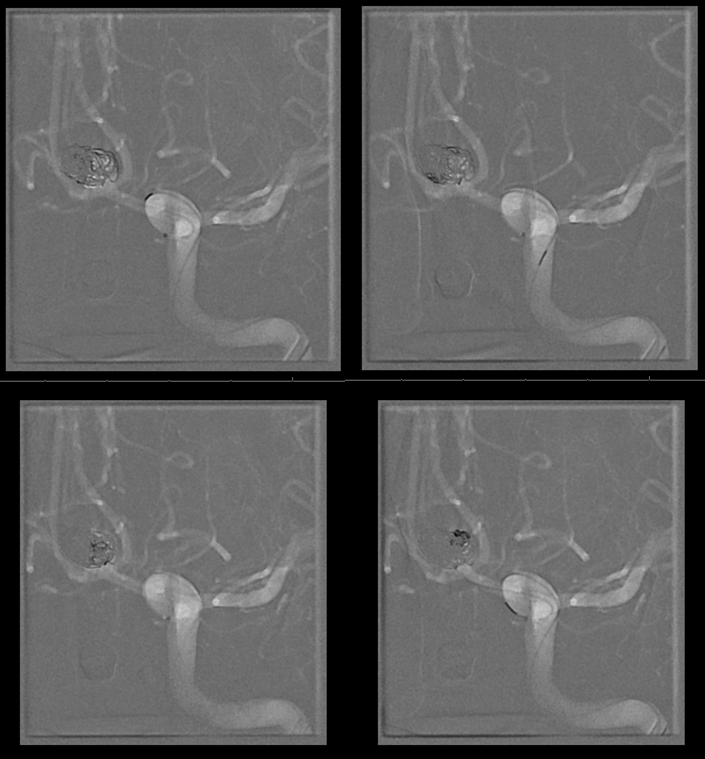
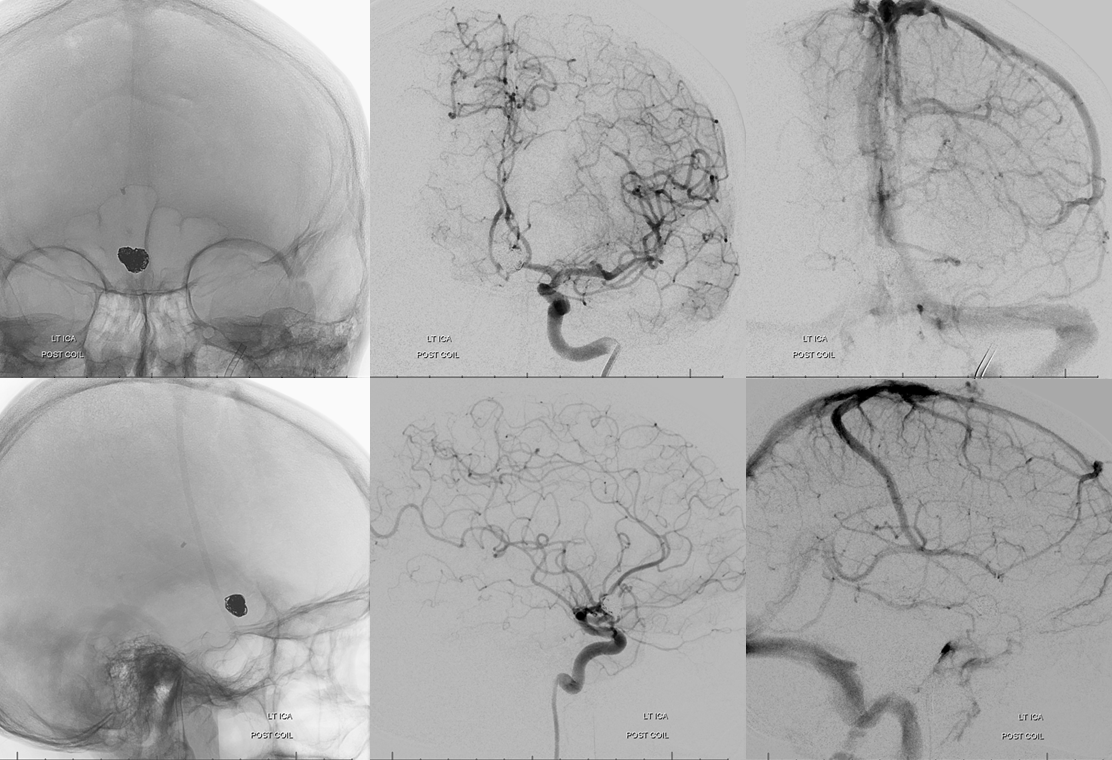
Post coil working projection. We were pretty happy at this point, even though this is partial treatment with pretty much zero chance of durability, and will require definitive management at a later time
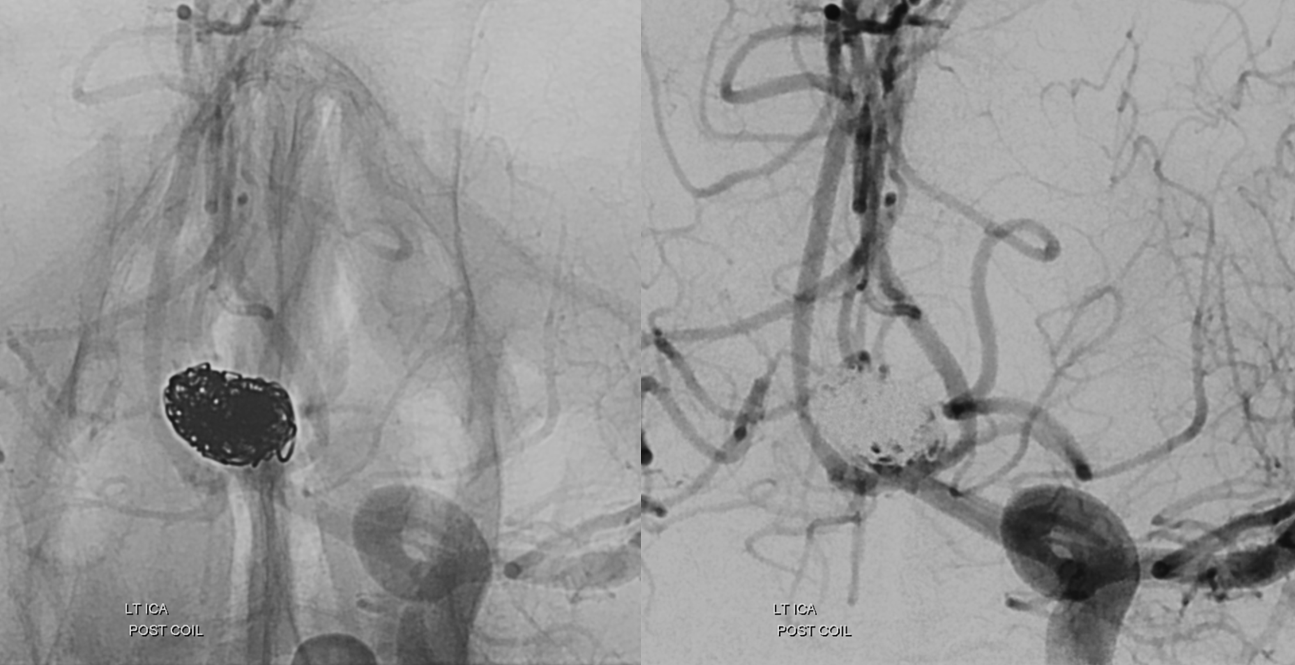
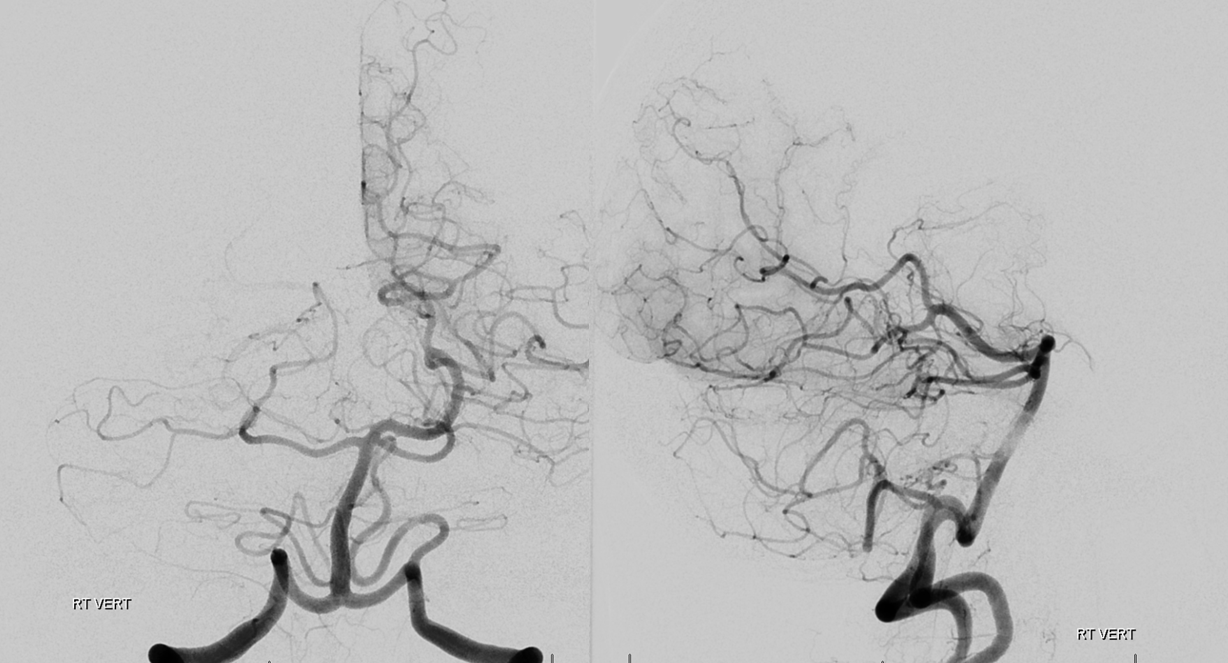
Global post
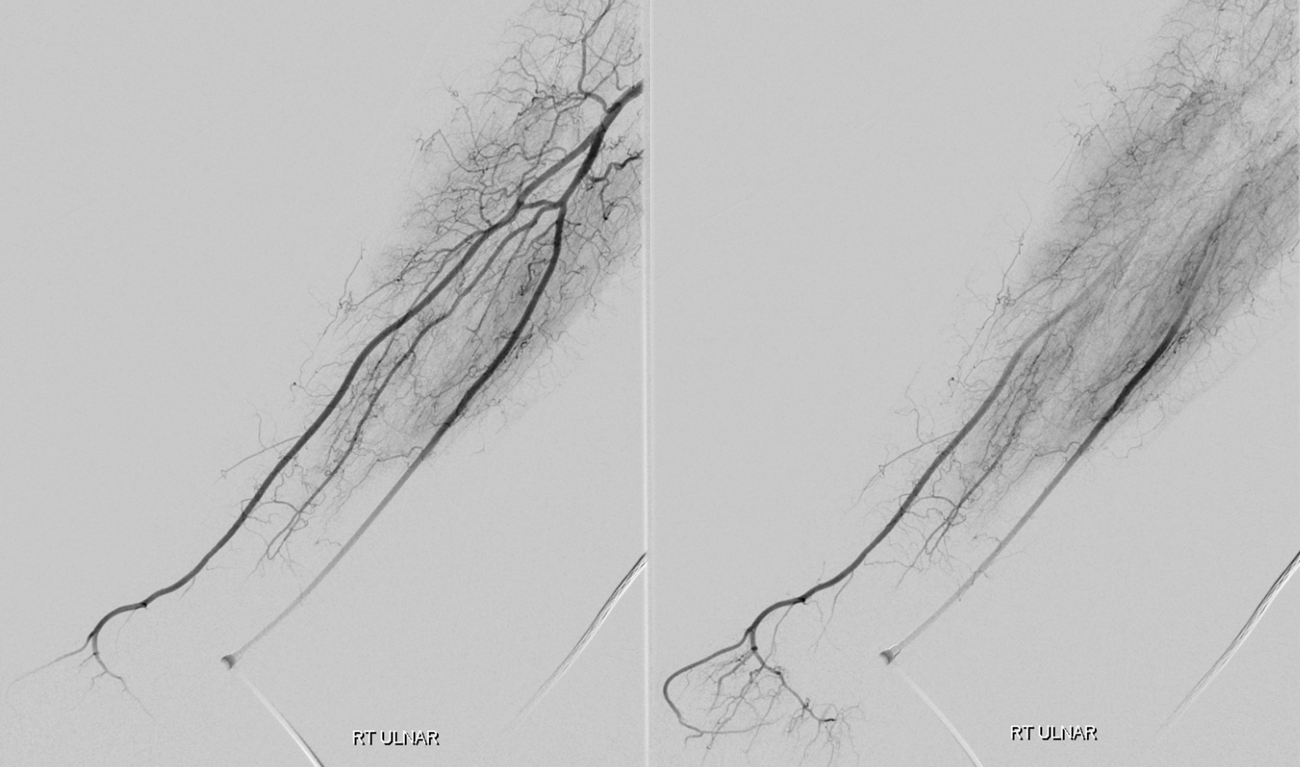
Brachial post
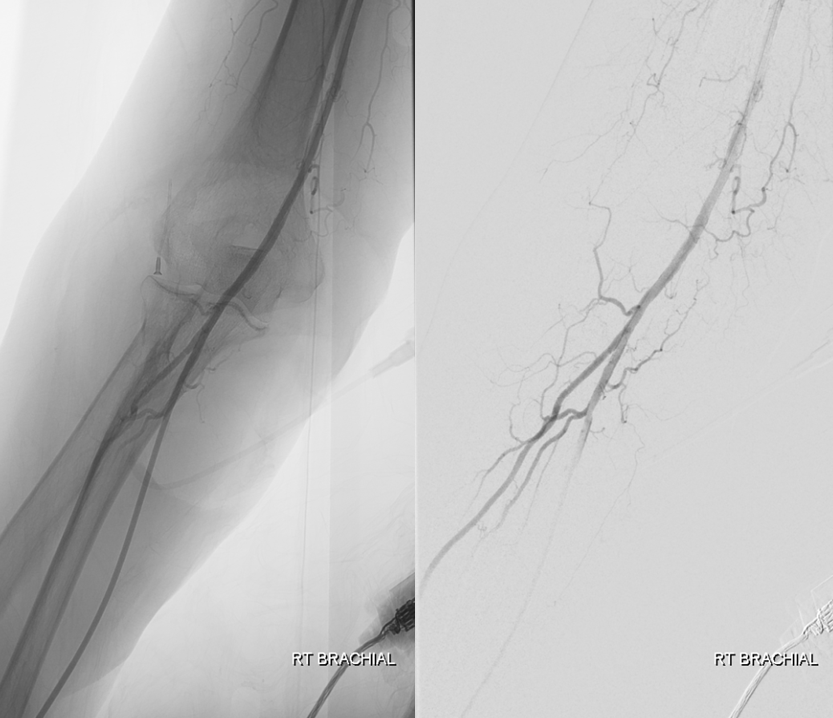
Brachial runoff. Radial is patent with a nice palmar arch
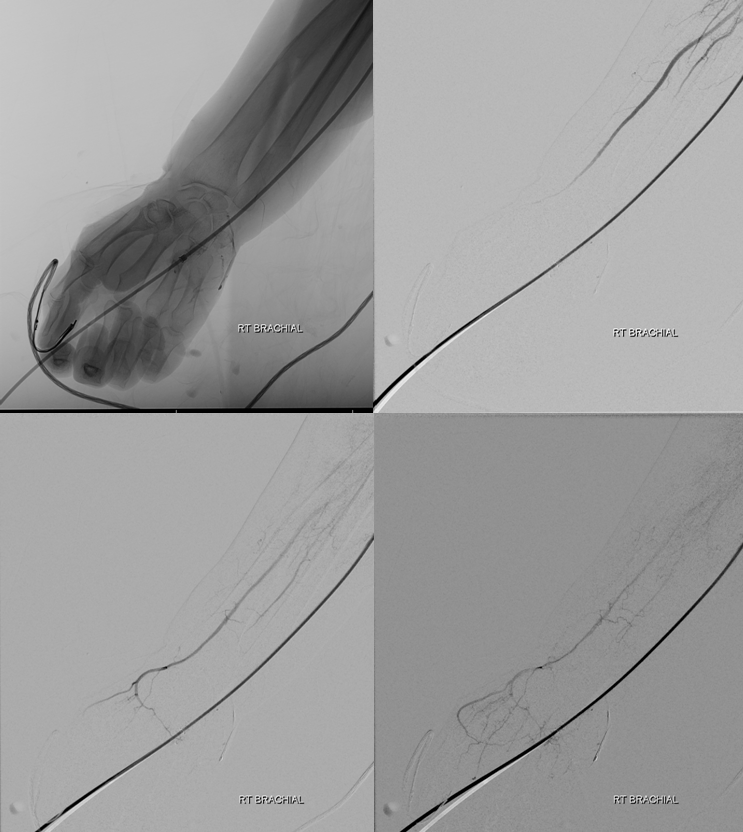
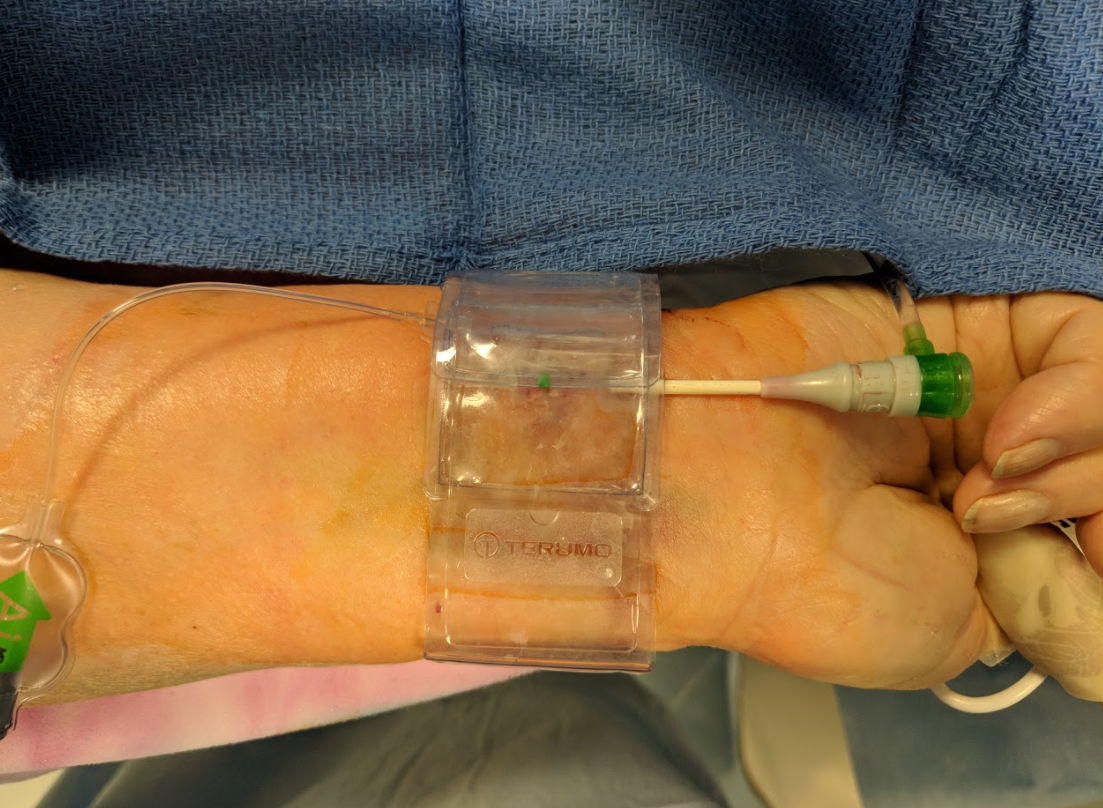
At conclusion, Trans”radial” band is on the ulnar side
Further reading:
https://www.ncbi.nlm.nih.gov/pubmed/26332022
Other Radial Artery cases on the “Cases” page