
Part of Technique Series
Recognizing a big embolus is easy. Small ones are harder to pick up. Truncated branch is an obvious clue. A better one, often, is evidence of collateral reconstitution of the occluded branch. This is a patient with a large left parietal convexity meningioma, for preoperative angiography and possible embolization
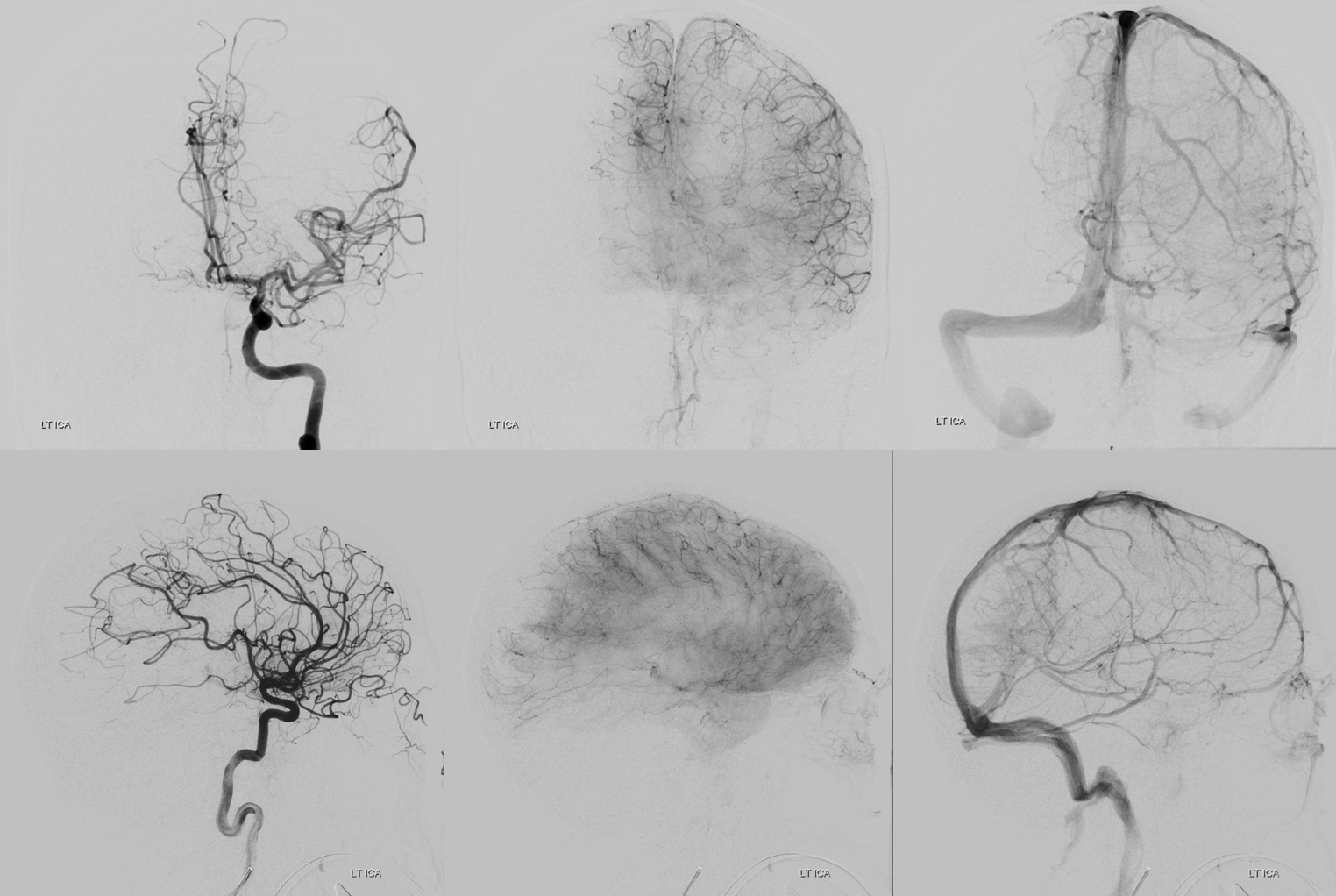
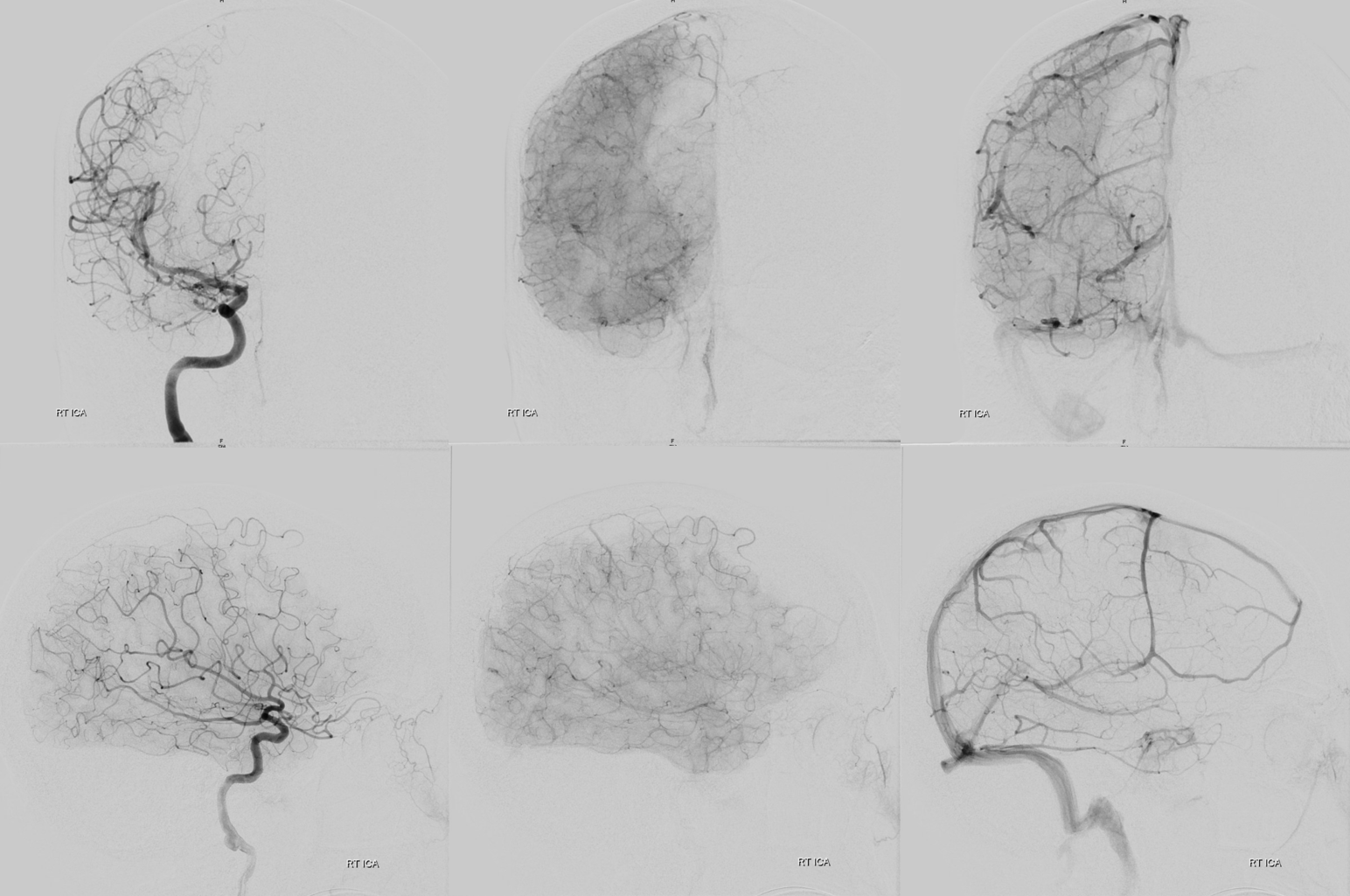
Pre-embo left ICA — note mass effect and pial tumor supply
Pre-embo right CCA — just to make it more difficult — the right pre-embo is a common injection
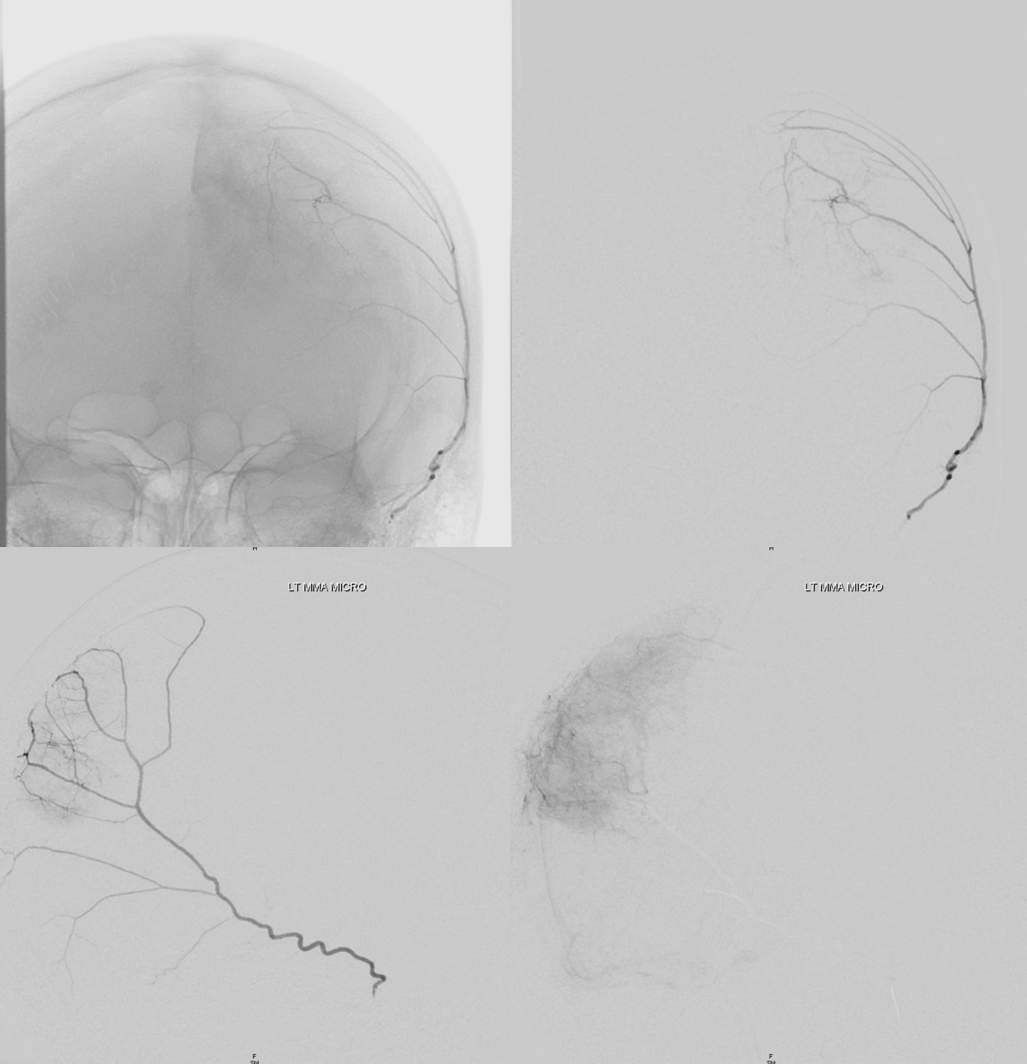
Left MMA — there is a variant here — the frontal branch of MMA is supplied by the left ophthalmic artery — note this above. More on this variant on the ophthalmic artery page
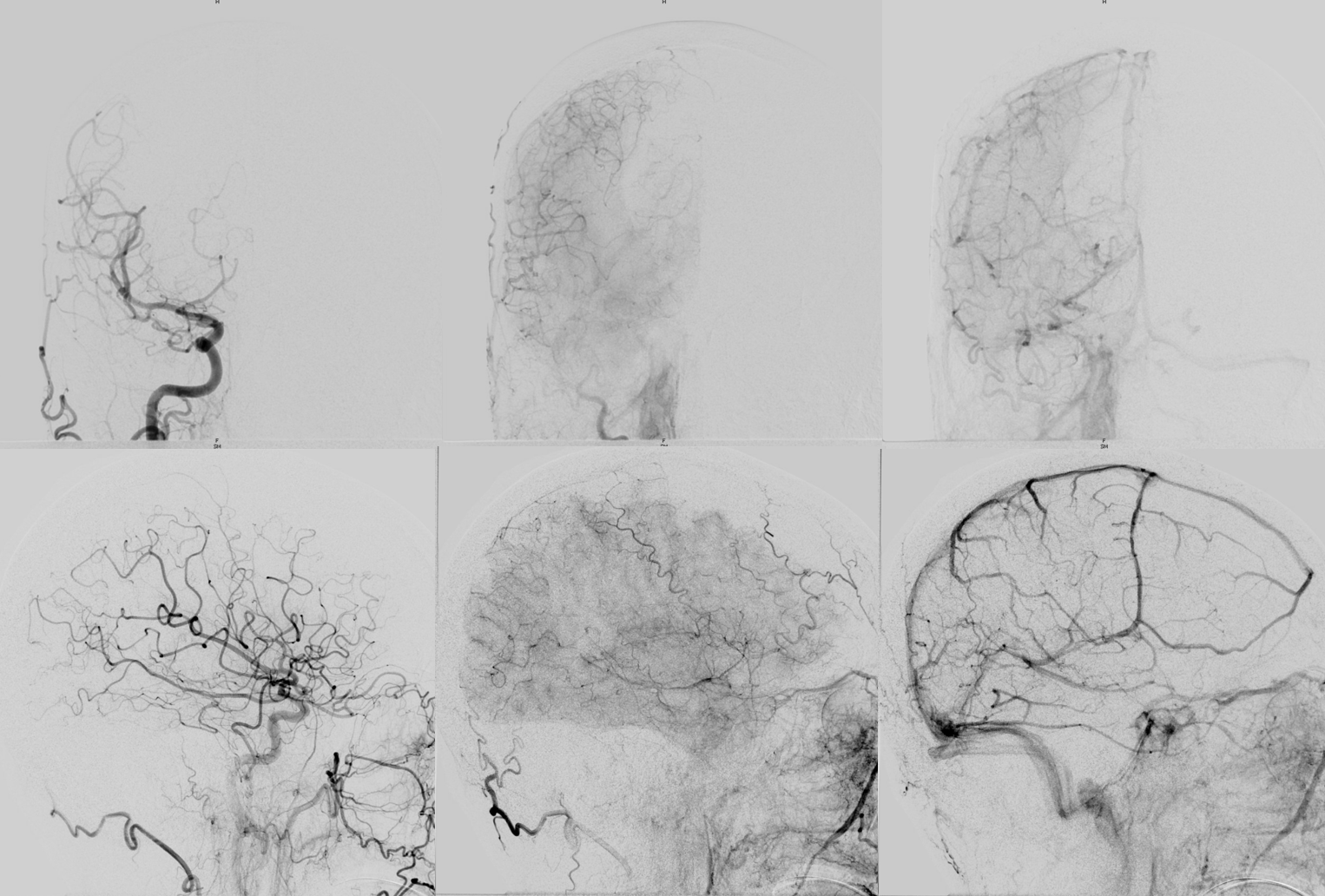
ICA post-left MMA embo — see frontal MMA branch? Do u see anything else? Its hard
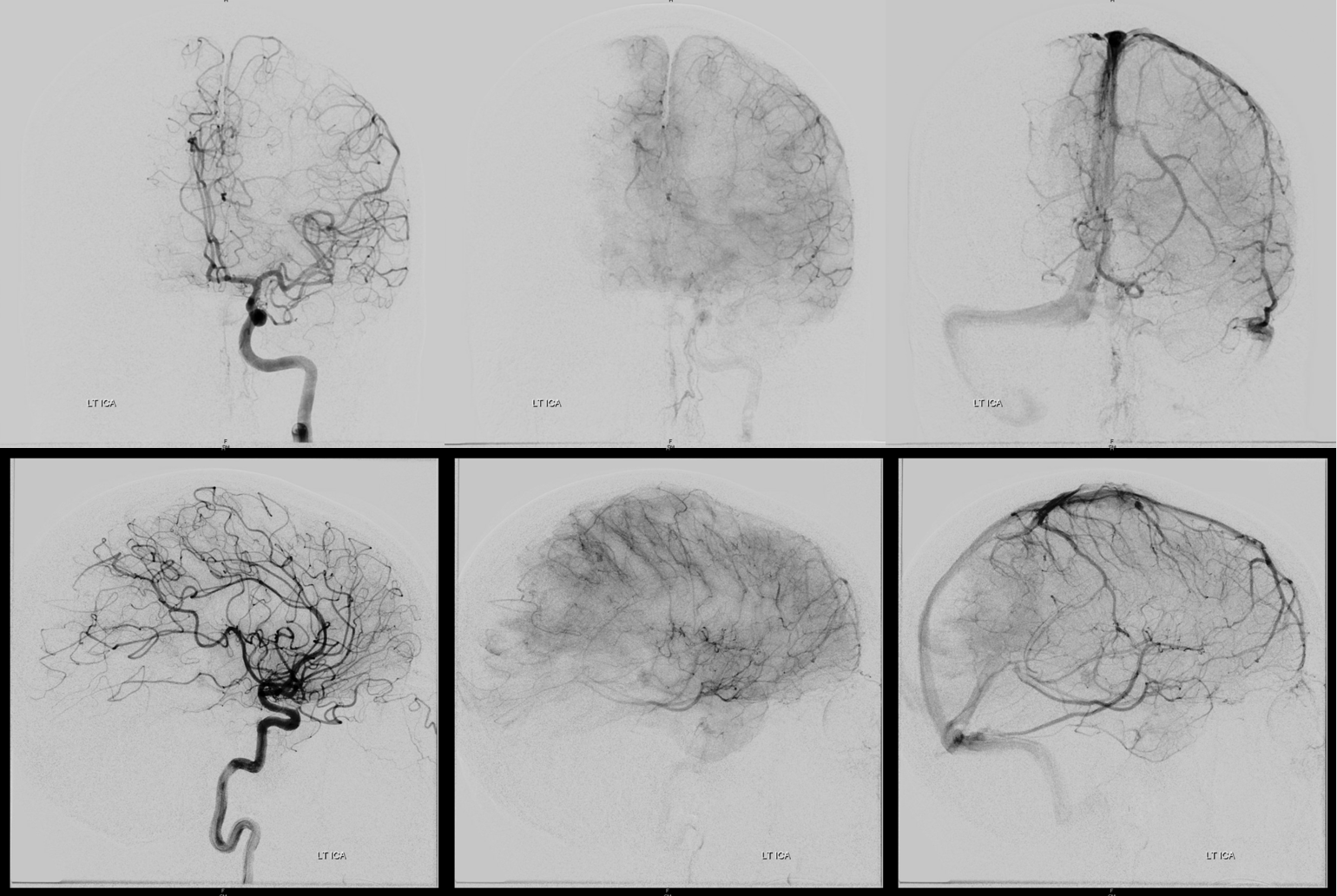
Post-embo right ICA — see the problem?
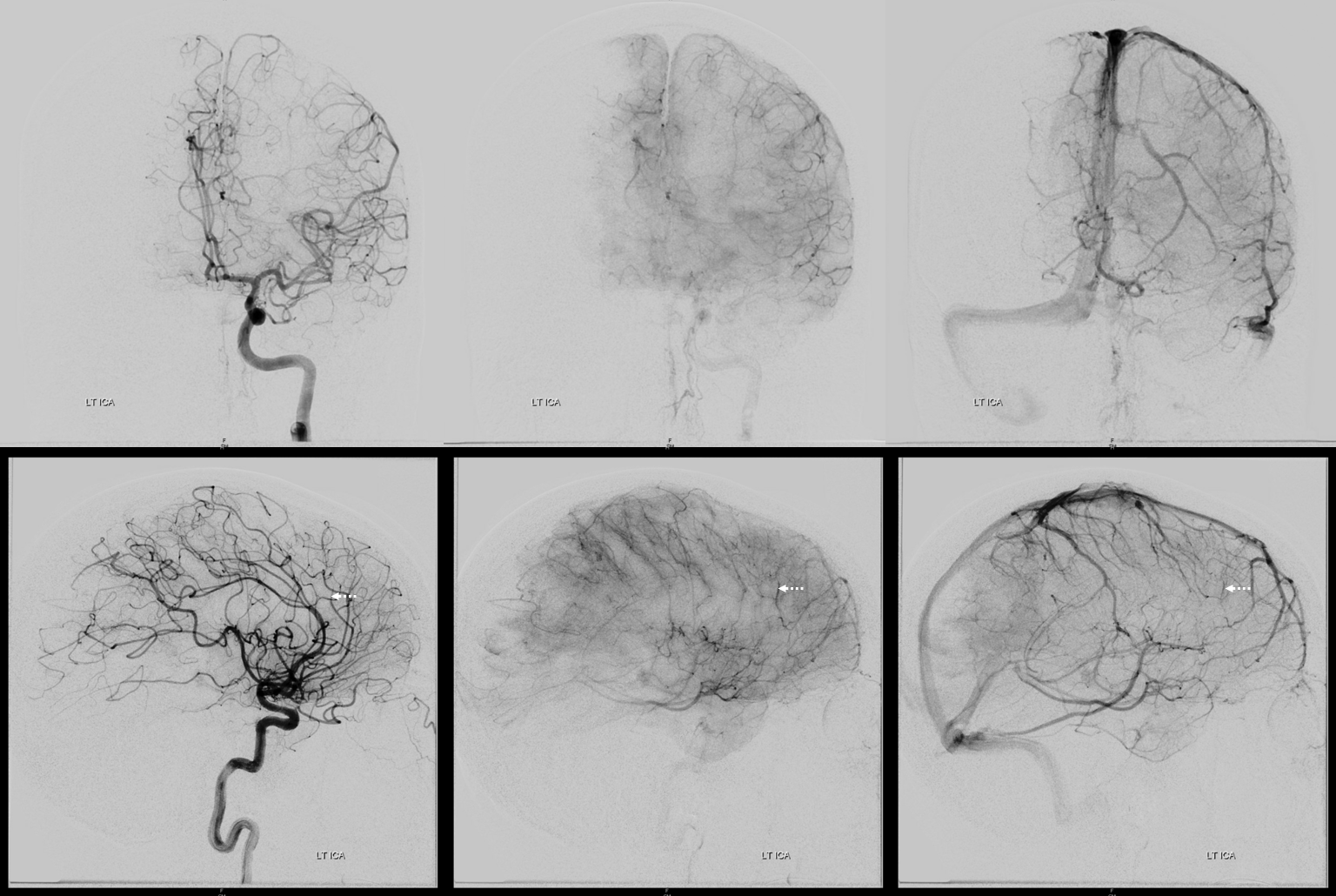
Below is the answer: There is an embolus in the ACA territory (dashed arrows) — its hard to recognize, because its small. There is a branch occlusion with arterial stump persisting in the venous phase
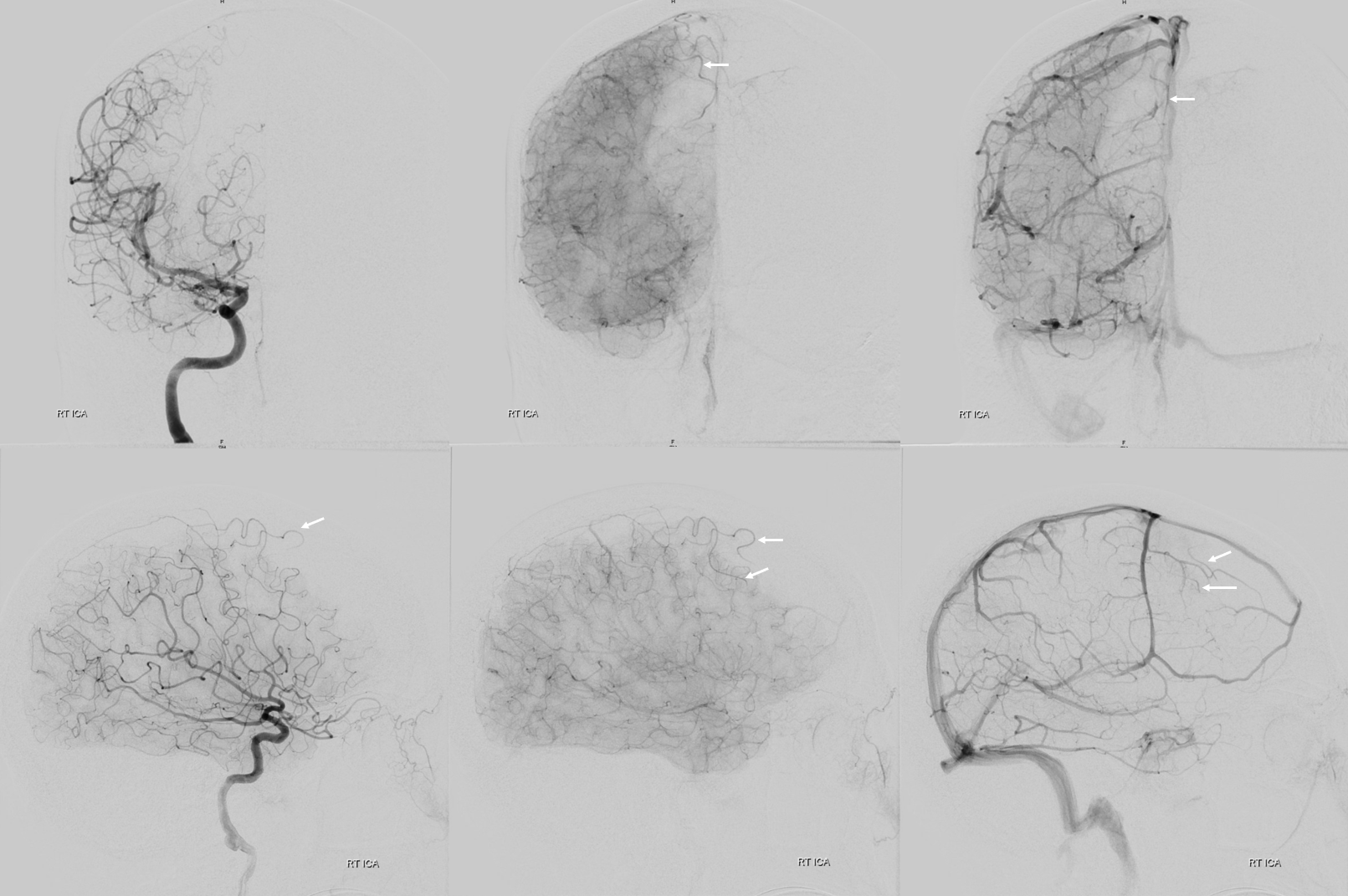
The right ICA injection is actually easier to interpret — there are strange-looking branches (white arrows) that were not there before — made easier to see because A1 is hypoplastic. They are ACA branches, downstream of the occlusion, reconstituted by leptomeningeal collaterals from the right MCA. The occlusion is thus of the right mid-frontal branch of the ACA .
Before (left) and after (right) images side by side
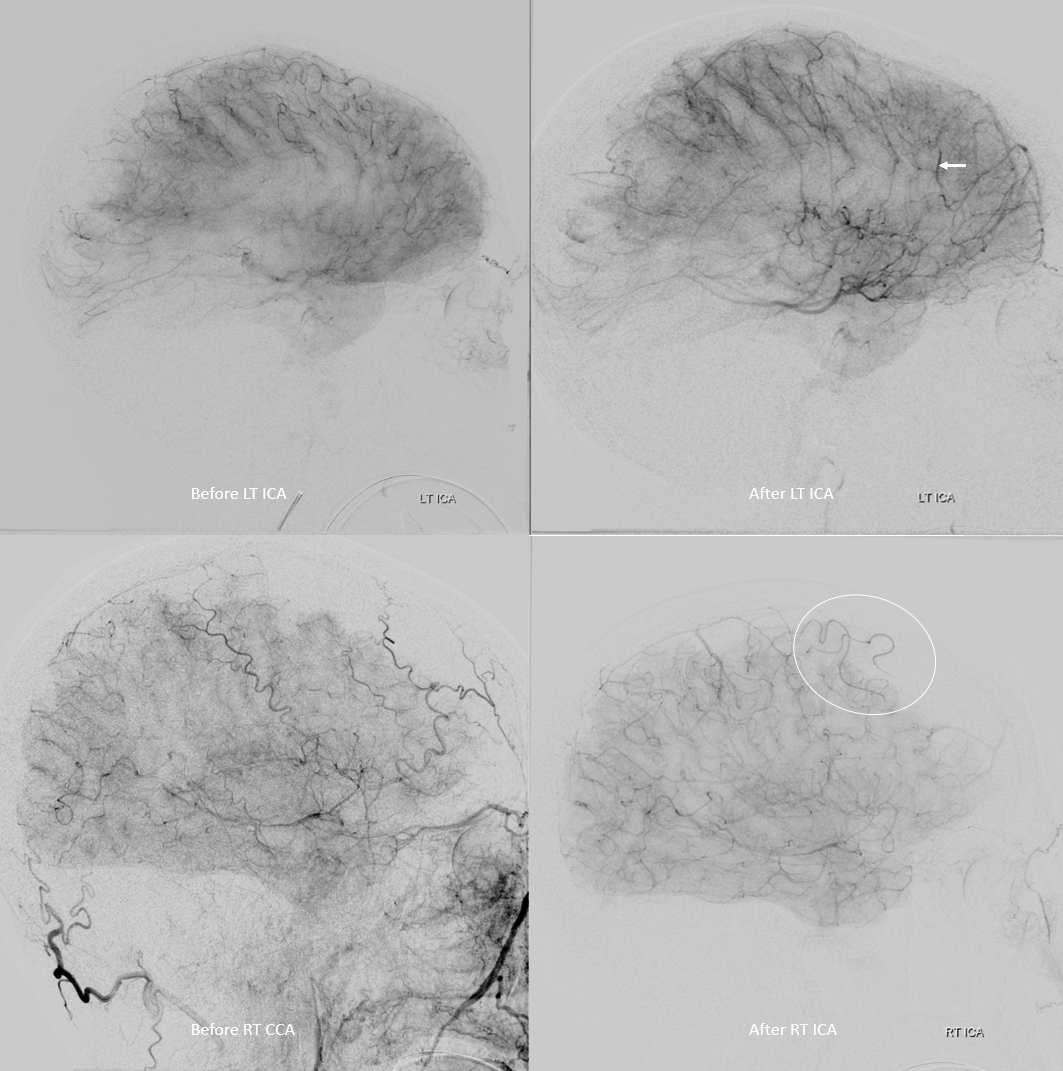
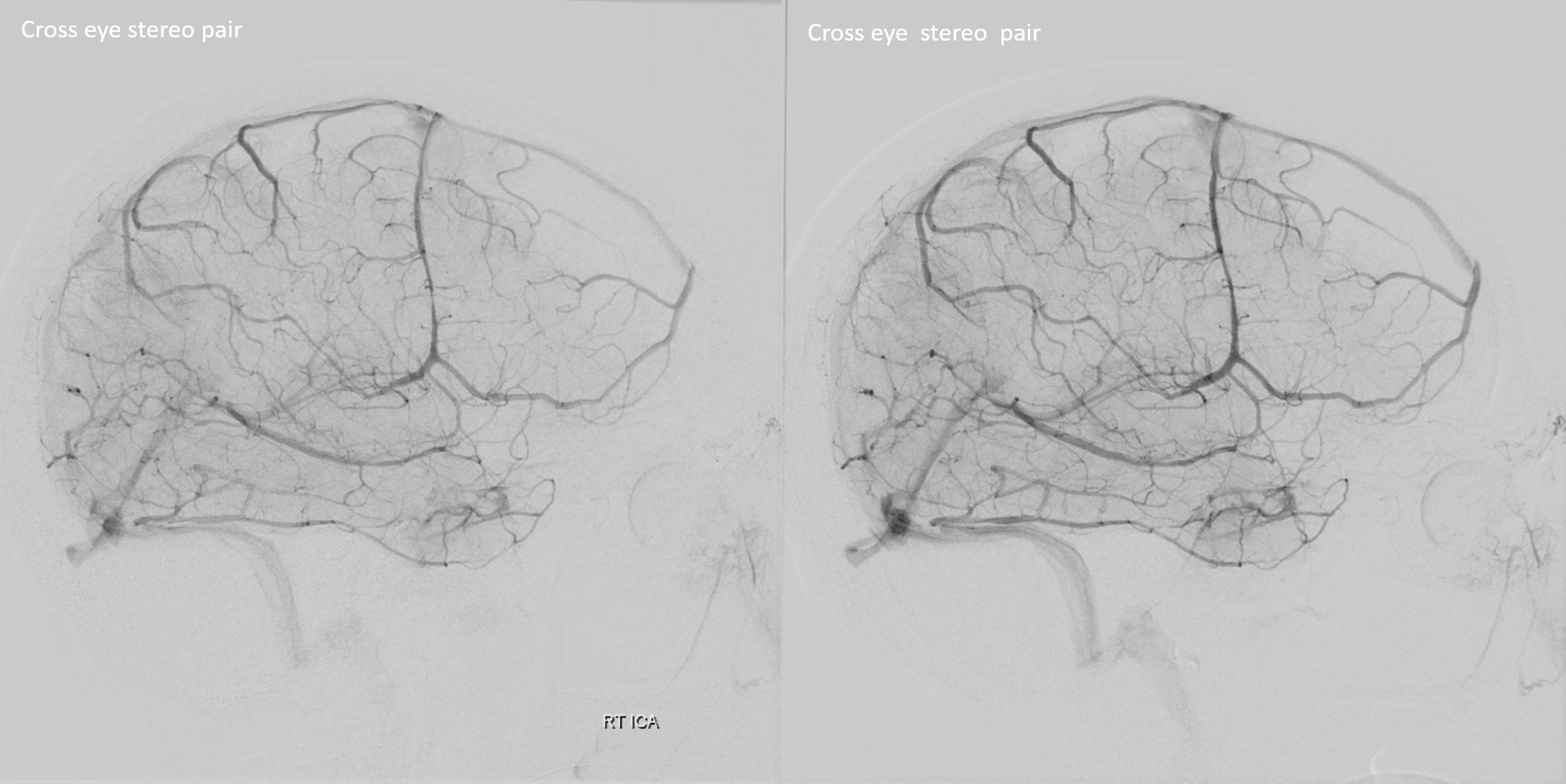
Stereo views, with reconstituted arteries in venous phase of normal brain.
Nothing was done, since the occlusion was in a “silent” part of brain, and no symptoms materialized. Given how slow the leptomeningeal reconstitution was, infraction should be expected.