
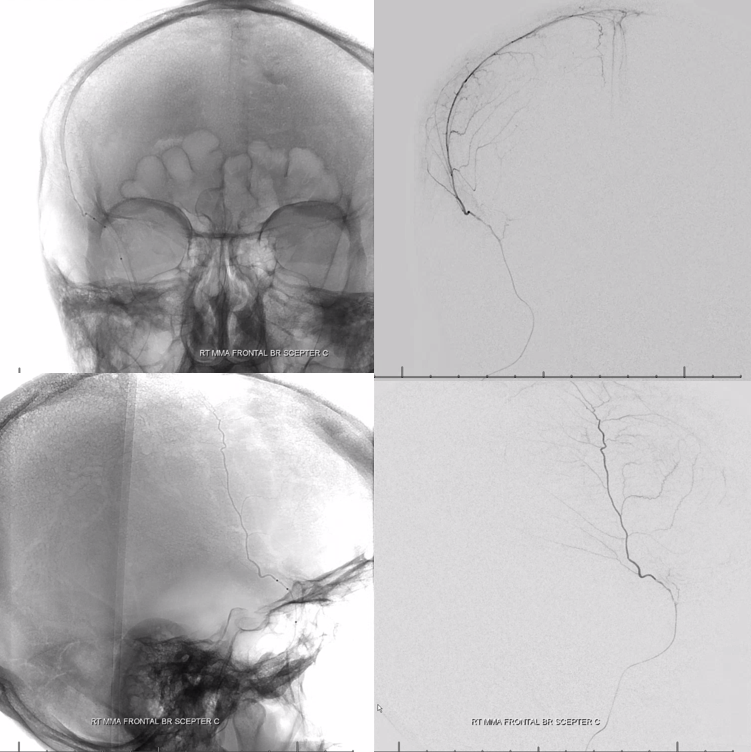
Probably nBCA is the least utilized agent for MMA embo. Its a shame — it works well, injections are quick, and can be very safe if one knows how to use it. For example, in this case of MMA supply to the orbit, glue is an excellent choice. Not what many would think, but true
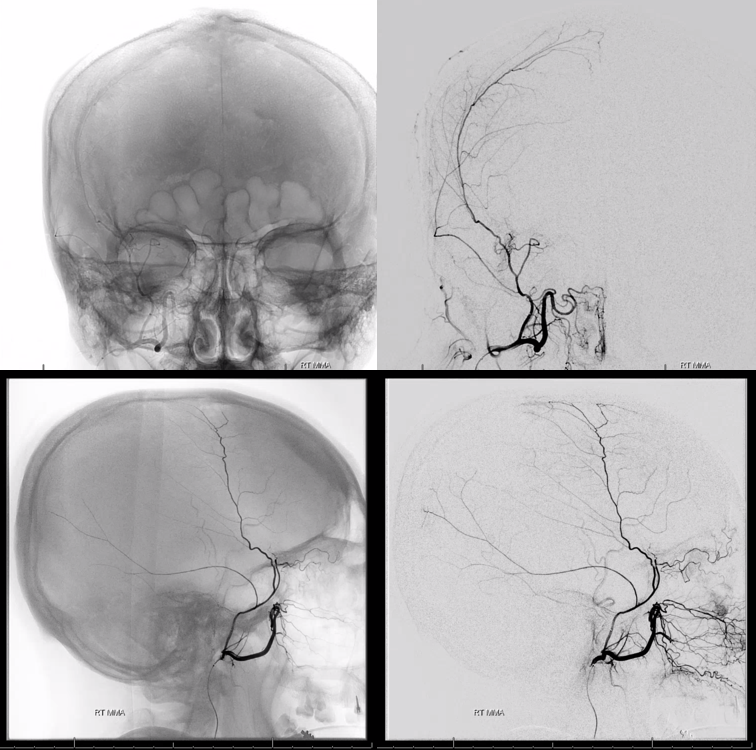
Frontal MMA meningolacrimal branch supply to orbit — notice medial entry into orbit
VR

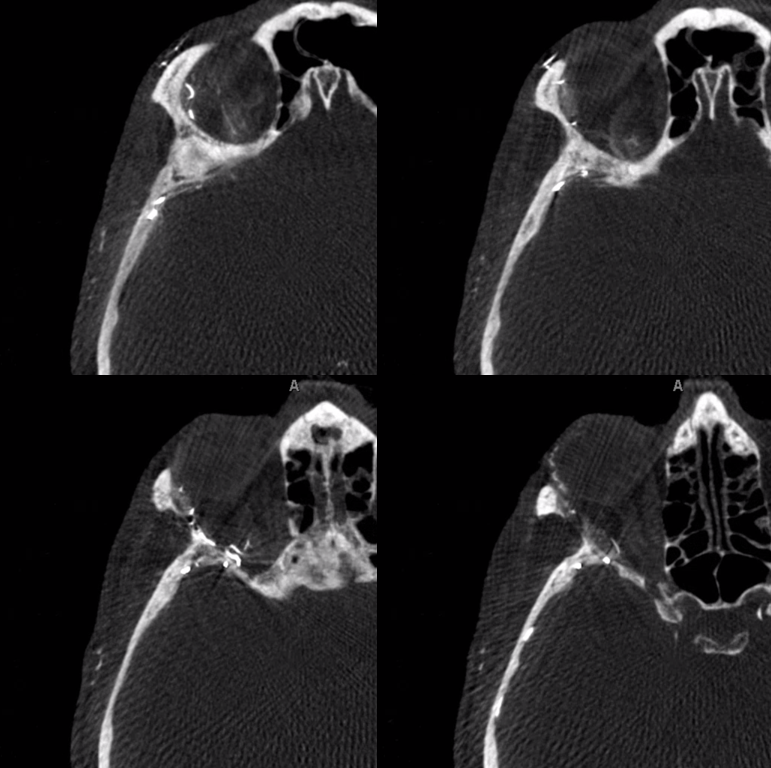
MIPS show superior orbital fissure entry site. Supply to superior rectus also
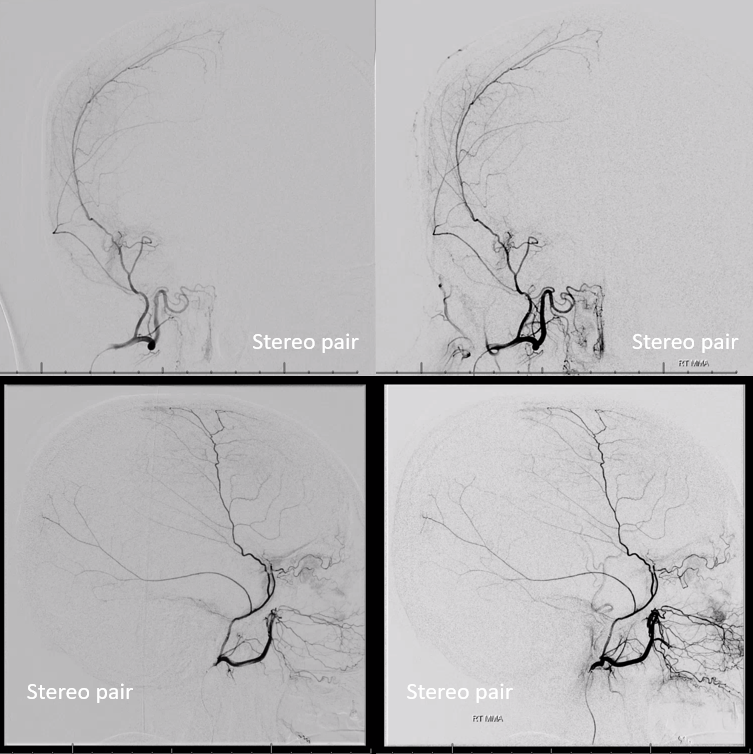
Stereos
What to do — go distal to the meningolacrimal branch with a scepter C
Late phase
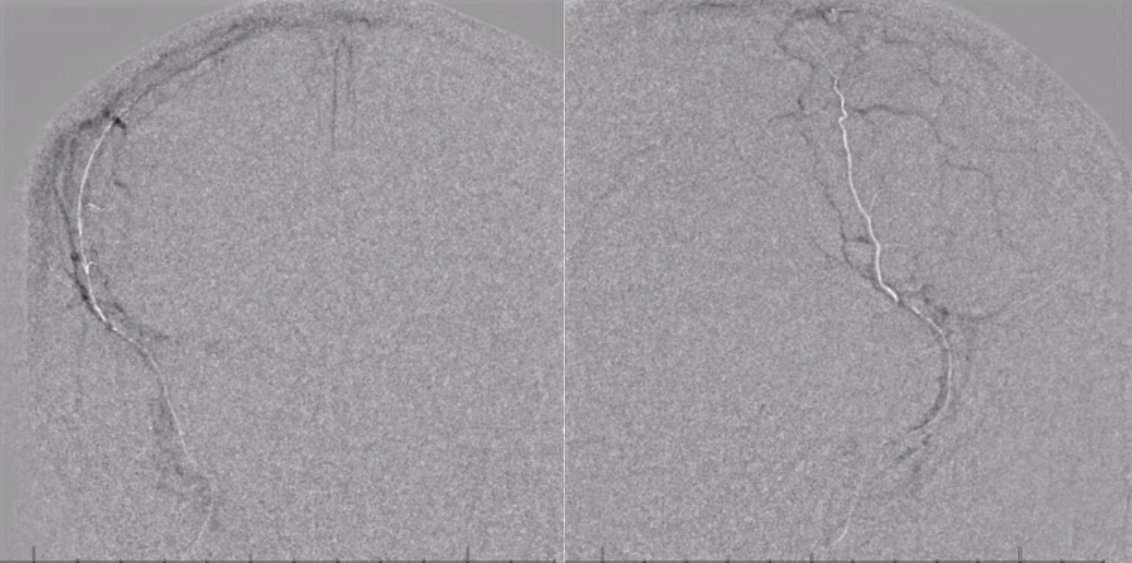
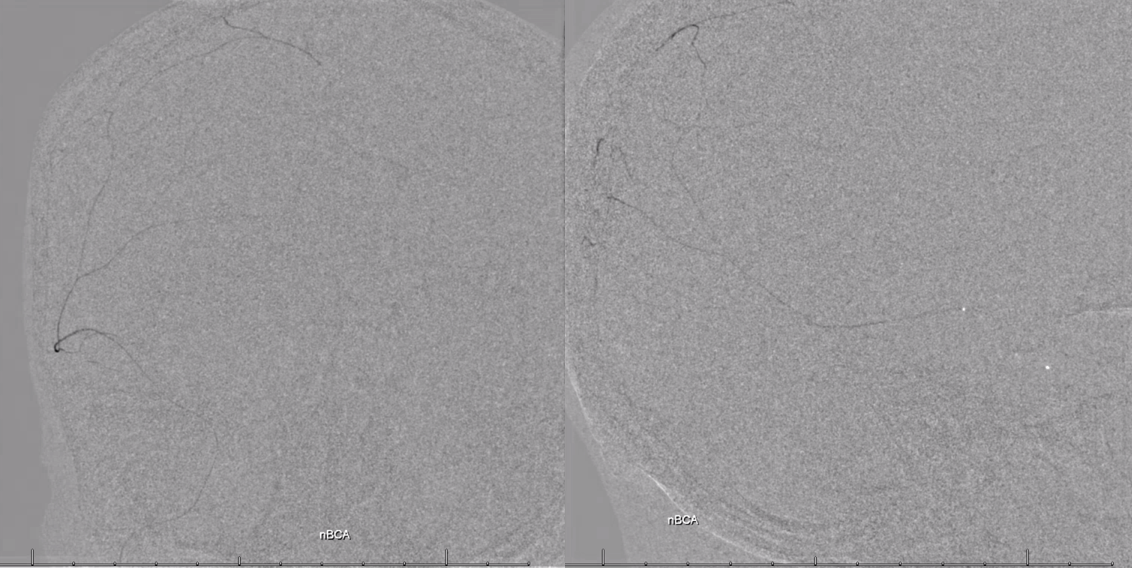
Now inflate the scepter gently but effectively to stop reflux, and inject 2:1 Lipidol:nBCA — excellent penetration into secondary MMA branches and the anterior falcine / anterior meningeal branch in wall of the superior sagittal sinus. Scepter ensures no reflux into the orbit
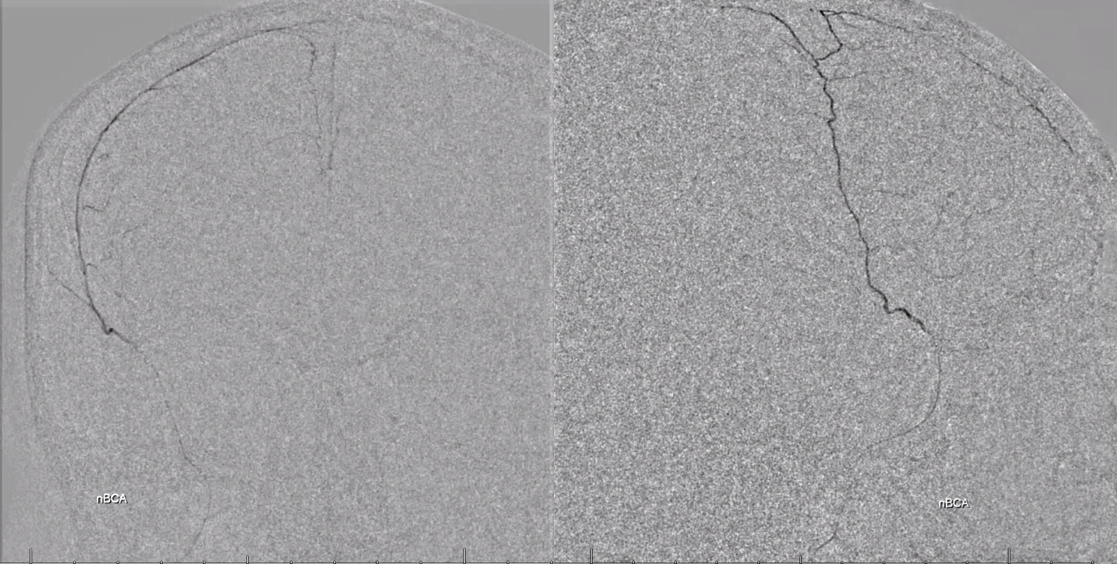
Now for the petrosquamosal branch — headway duo catheterization of smaller branch achieves flow control
nBCA here — nice penetration even beyond midline — a potential collateral pathway for mma reconstitution is contralateral MMA
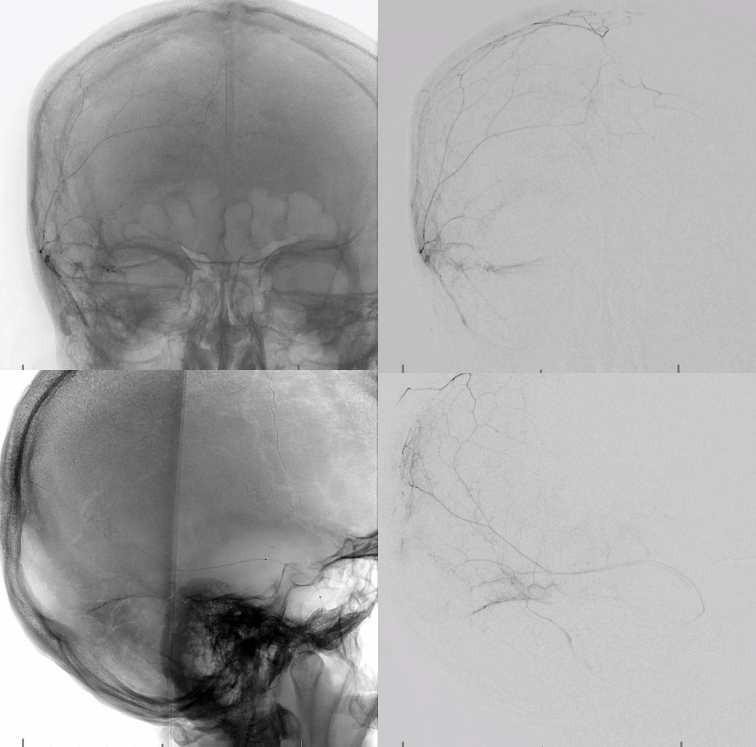
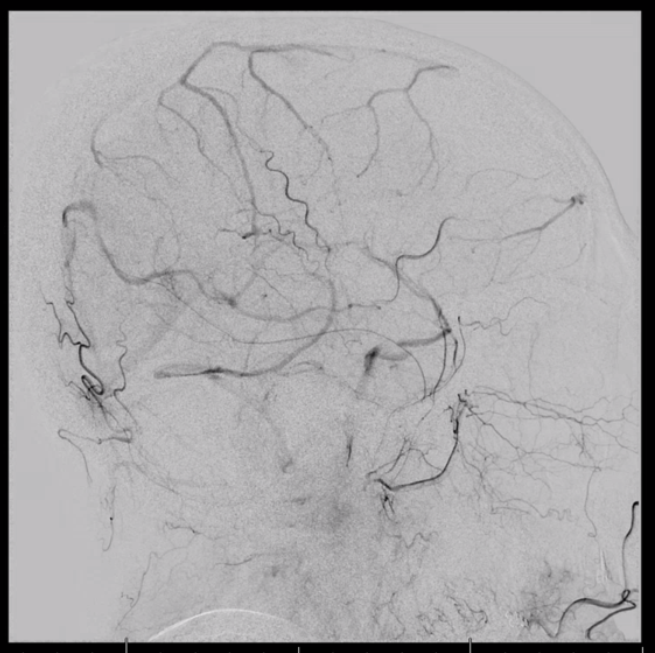
Post embo shows preserved meningolactrimal branch
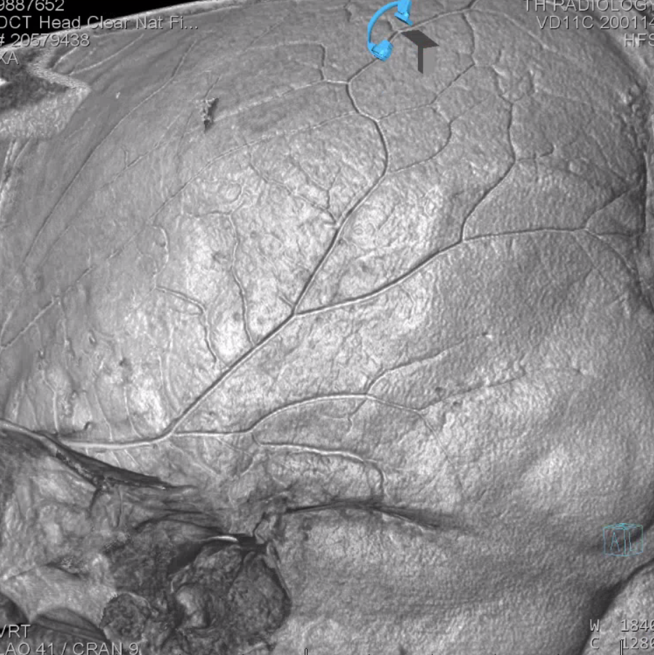
Cast of nBCA inside convexity on DYNA CT — nice, right?
More MMA embo cases on Case Archive page